

SynCardia: the total artificial heart
- PMID: 25512904
- PMCID: PMC4250553
- DOI: 10.3978/j.issn.2225-319X.2014.11.07
SynCardia: the total artificial heart
Abstract
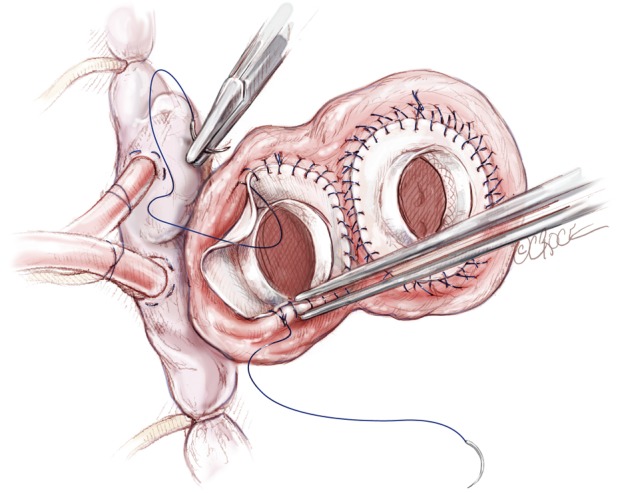
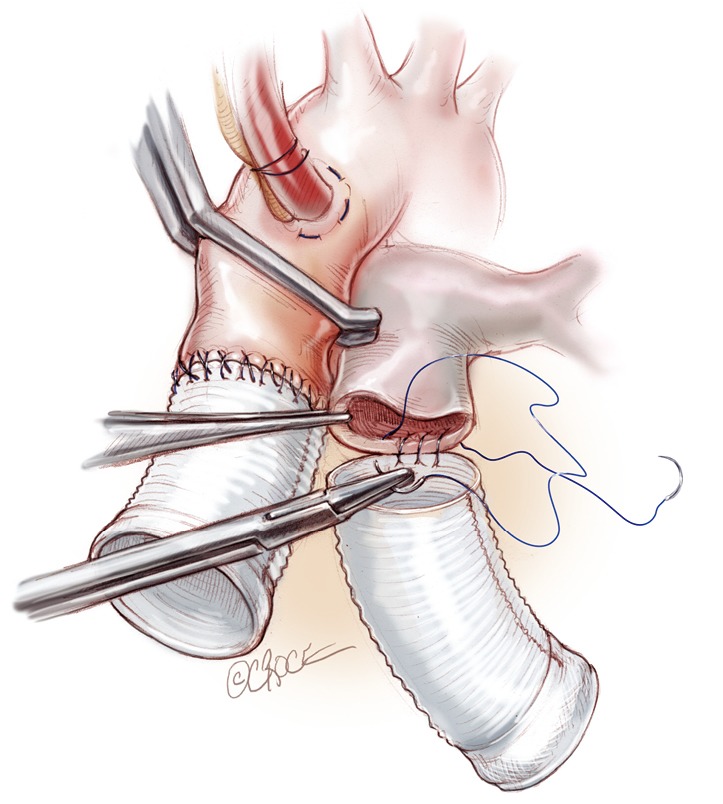
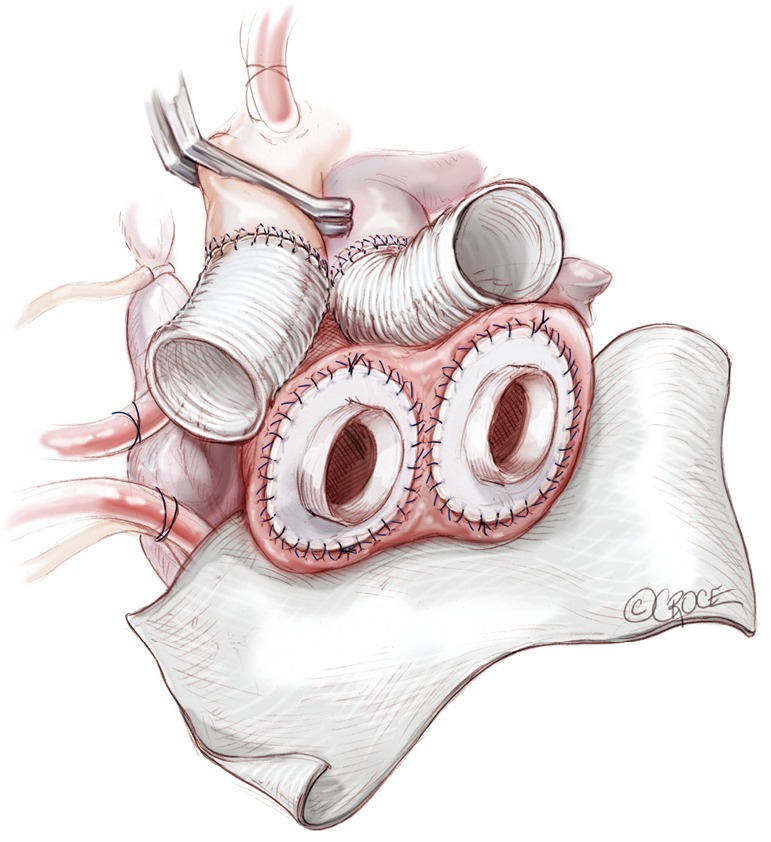
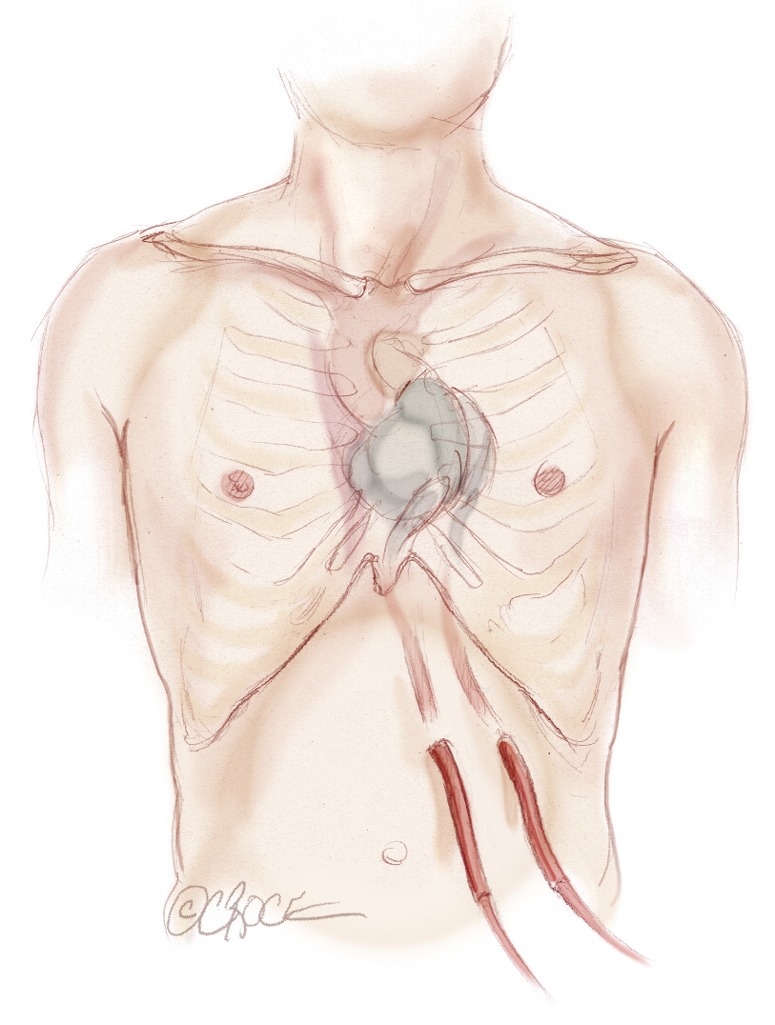
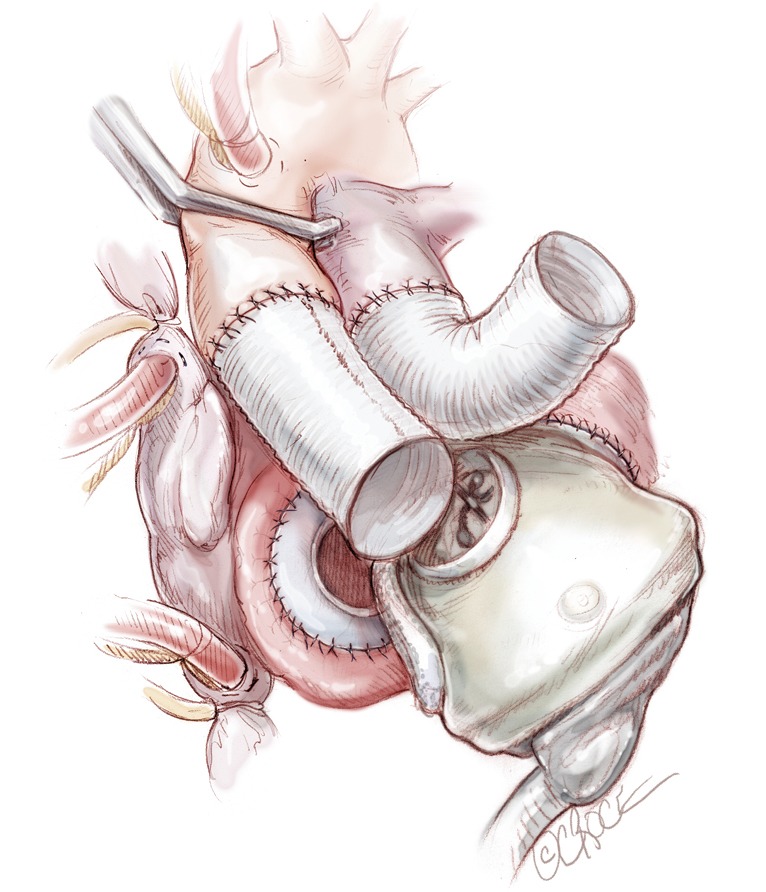
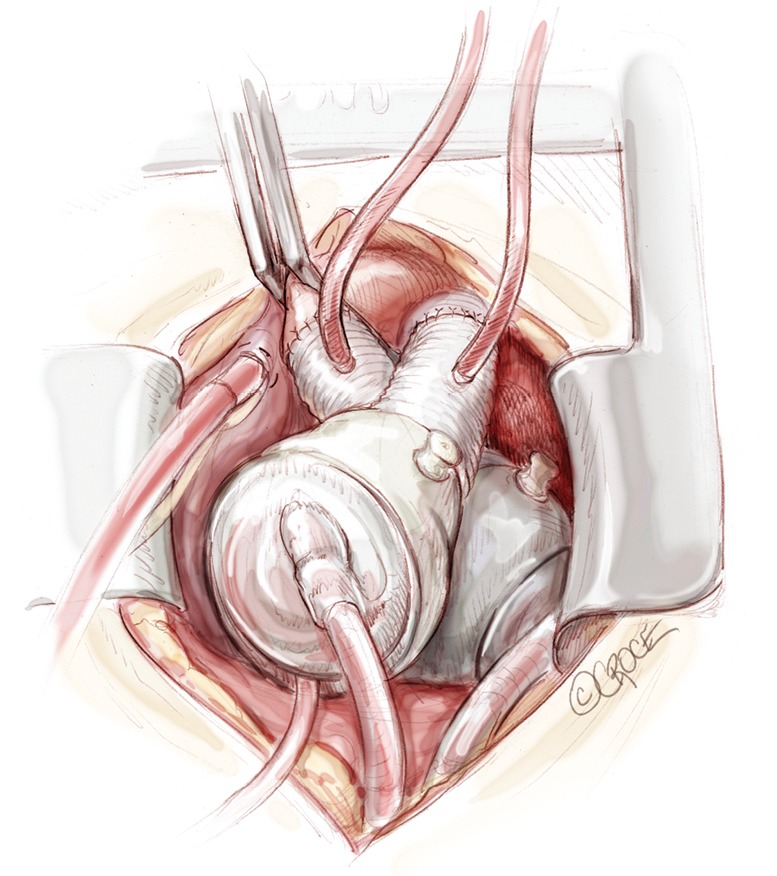
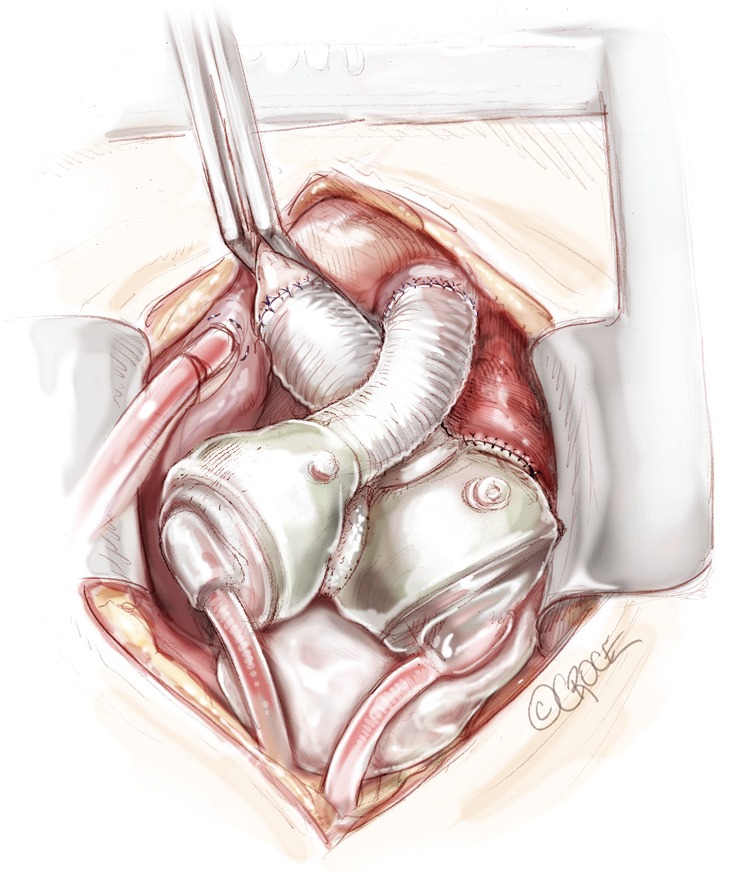
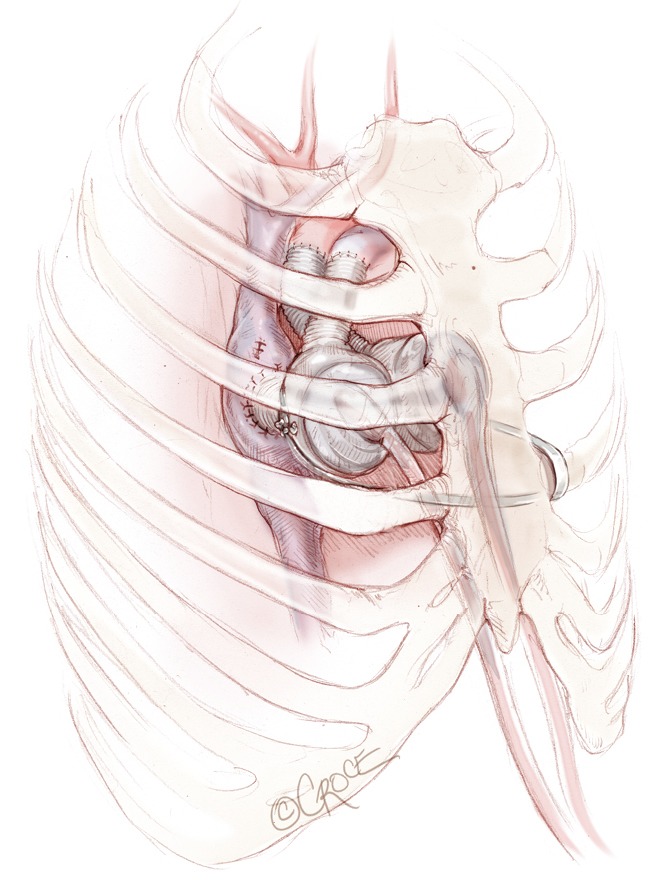
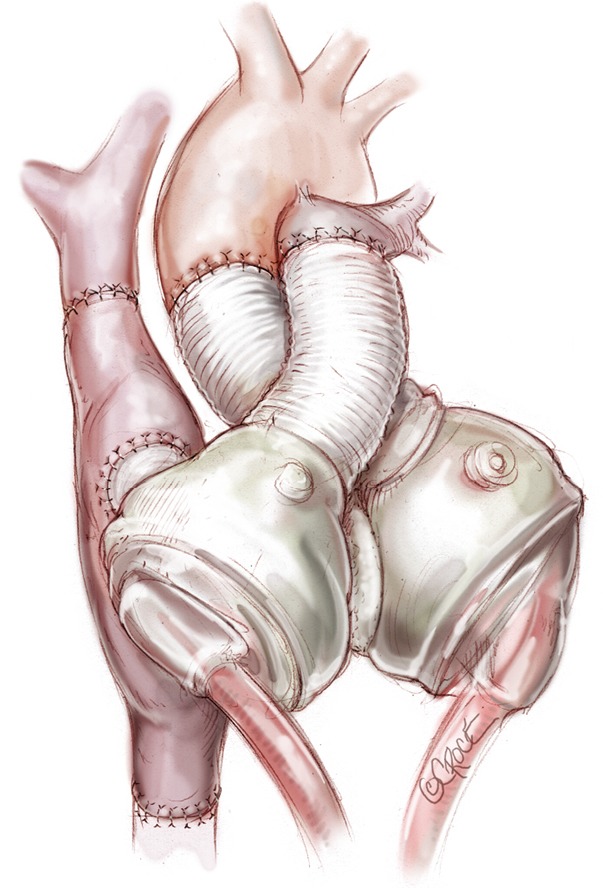
The SynCardia total artificial heart (TAH) currently provides the most definitive option for patients with biventricular failure who are not candidates for isolated left ventricular (LV) assist device placement. The techniques for implantation are adaptable to almost all patients with advanced heart failure, including those with severe biventricular cardiomyopathy, complex congenital heart disease, failed LV assist devices, failed transplantations, and acquired structural heart defects that have failed or are not amenable to conventional surgical treatment. Over the years, the implantation technique has evolved in order to minimize the surgical invasiveness of the procedure, in anticipation of additional future surgery. Meticulous hemostasis with double layer sutures, use of Gore-Tex sheets around the TAH and the pericardial cavity, and use of tissue expanders to avoid contraction of pericardial cavity around the device are discussed in detail in the following report. Additionally, we will provide our experience with implantation of TAH in various challenging scenarios, such as patients with a small chest cavity, congenital heart defects, and simultaneous use of extracorporeal membrane oxygenation (ECMO).
Keywords: SynCardia; Total artificial heart (TAH); cardiowest; implantation technque.
Figures
References
-
- DeVries WC, Anderson JL, Joyce LD, et al. Clinical use of the total artificial heart. N Engl J Med 1984;310:273-8. - PubMed
-
- El-Banayosy A, Arusoglu L, Morshuis M, et al. CardioWest total artificial heart: Bad Oeynhausen experience. Ann Thorac Surg 2005;80:548-52. - PubMed
-
- Copeland JG, Smith RG, Arabia FA, et al. Cardiac replacement with a total artificial heart as a bridge to transplantation. N Engl J Med 2004;351:859-67. - PubMed
-
- Copeland JG, Copeland H, Gustafson M, et al. Experience with more than 100 total artificial heart implants. J Thorac Cardiovasc Surg 2012;143:727-34. - PubMed
-
- Kirsch ME, Nguyen A, Mastroianni C, et al. SynCardia temporary total artificial heart as bridge to transplantation: current results at la pitié hospital. Ann Thorac Surg 2013;95:1640-6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources