

An Integrative Model of Physiological Traits Can be Used to Predict Obstructive Sleep Apnea and Response to Non Positive Airway Pressure Therapy
- PMID: 25515107
- PMCID: PMC4434563
- DOI: 10.5665/sleep.4750
An Integrative Model of Physiological Traits Can be Used to Predict Obstructive Sleep Apnea and Response to Non Positive Airway Pressure Therapy
Abstract
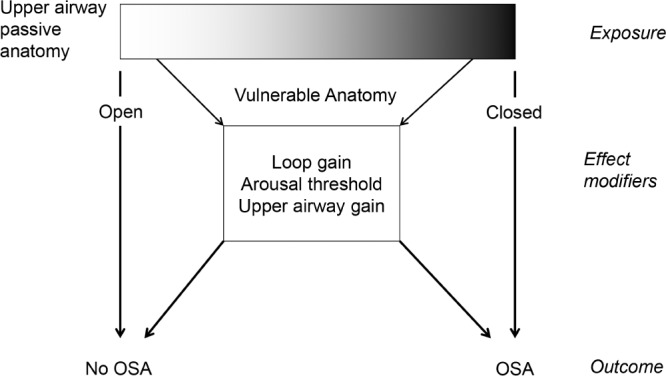
Study objectives: Both anatomical and nonanatomical traits are important in obstructive sleep apnea (OSA) pathogenesis. We have previously described a model combining these traits, but have not determined its diagnostic accuracy to predict OSA. A valid model, and knowledge of the published effect sizes of trait manipulation, would also allow us to predict the number of patients with OSA who might be effectively treated without using positive airway pressure (PAP).
Design, participants and intervention: Fifty-seven subjects with and without OSA underwent standard clinical and research sleep studies to measure OSA severity and the physiological traits important for OSA pathogenesis, respectively. The traits were incorporated into a physiological model to predict OSA. The model validity was determined by comparing the model prediction of OSA to the clinical diagnosis of OSA. The effect of various trait manipulations was then simulated to predict the proportion of patients treated by each intervention.
Measurements and results: The model had good sensitivity (80%) and specificity (100%) for predicting OSA. A single intervention on one trait would be predicted to treat OSA in approximately one quarter of all patients. Combination therapy with two interventions was predicted to treat OSA in ∼50% of patients.
Conclusions: An integrative model of physiological traits can be used to predict population-wide and individual responses to non-PAP therapy. Many patients with OSA would be expected to be treated based on known trait manipulations, making a strong case for the importance of non-anatomical traits in OSA pathogenesis and the effectiveness of non-PAP therapies.
Keywords: arousal threshold; non PAP therapy; obstructive sleep apnea; upper airway anatomy.
© 2015 Associated Professional Sleep Societies, LLC.
Figures
References
-
- Smith PL, Wise RA, Gold AR, Schwartz AR, Permutt S. Upper airway pressure-flow relationships in obstructive sleep apnea. J Appl Physiol. 1988;64:789–95. - PubMed
-
- White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med. 2005;172:1363–70. - PubMed
-
- Younes M, Ostrowski M, Thompson W, Leslie C, Shewchuk W. Chemical control stability in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2001;163:1181–90. - PubMed
-
- Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS) Sleep Med Rev. 2003;7:81–99. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
