

Role of interventional radiology in the management of complications after pancreatic surgery: a pictorial review
- PMID: 25516470
- PMCID: PMC4376815
- DOI: 10.1007/s13244-014-0372-y
Role of interventional radiology in the management of complications after pancreatic surgery: a pictorial review
Abstract
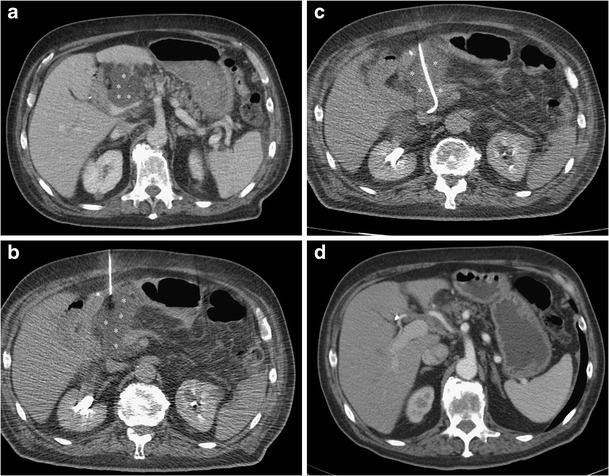
Pancreatic resections are surgical procedures associated with high incidence of complications, with relevant morbidity and mortality even at high volume centres. A multidisciplinary approach is essential in the management of these events and interventional radiology plays a crucial role in the treatment of patients developing post-surgical complications. This paper offers an overview on the interventional radiological procedures that can be performed to treat different type of complications after pancreatic resection. Procedures such as percutaneous drainage of fluid collections, percutaneous transhepatic biliary procedures, arterial embolisation, venous interventions and fistula embolisation are viable treatment options, with fewer complications compared with re-look surgery, shorter hospital stay and faster recovery. A selection of cases of complications following pancreatic surgery managed with interventional radiological procedure are presented and discussed. Teaching Points • Interventional radiology is crucial to treat complications after pancreatic surgery • Percutaneous drainage of collections can be performed under ultrasound or computed tomography guidance • Percutaneous biliary procedures can be used to treat biliary complications • Venous procedures can be performed effectively through transhepatic or transjugular access • Fistulas can be treated effectively by percutaneous embolisation.
Figures





References
-
- Buchler MW, Wagner M, Schmied BM, Uhl W, Friess H, Z’Graggen K (2003) Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Arch Surg 138(12):1310–1314 - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL et al (2000) Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg 4(6):567–579 - PubMed
-
- Gervais DA, Fernandez-del Castillo C, O’Neill MJ, Hahn PF, Mueller PR (2001) Complications after pancreatoduodenectomy: imaging and imaging-guided interventional procedures. Radiographics 21(3):673–690 - PubMed
-
- Zink SI, Soloff EV, White RR et al (2009) Pancreaticoduodenectomy: frequency and outcome of post-operative imaging-guided percutaneous drainage. Abdom Imaging 34(6):767–771 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
