

Current status of function-preserving surgery for gastric cancer
- PMID: 25516640
- PMCID: PMC4265587
- DOI: 10.3748/wjg.v20.i46.17297
Current status of function-preserving surgery for gastric cancer
Abstract
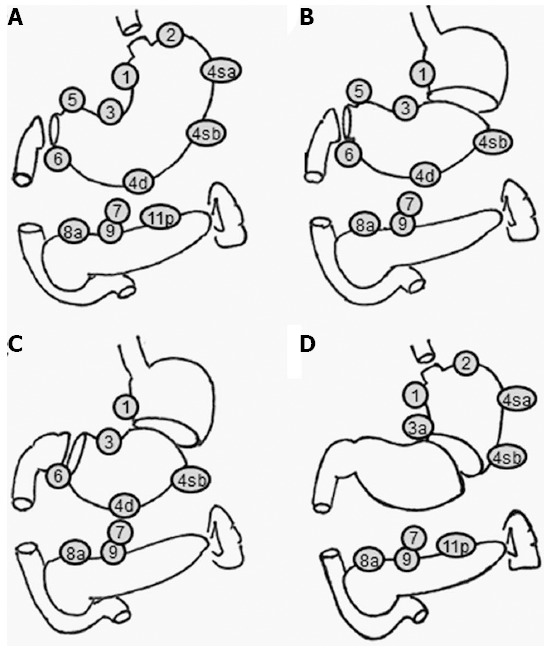
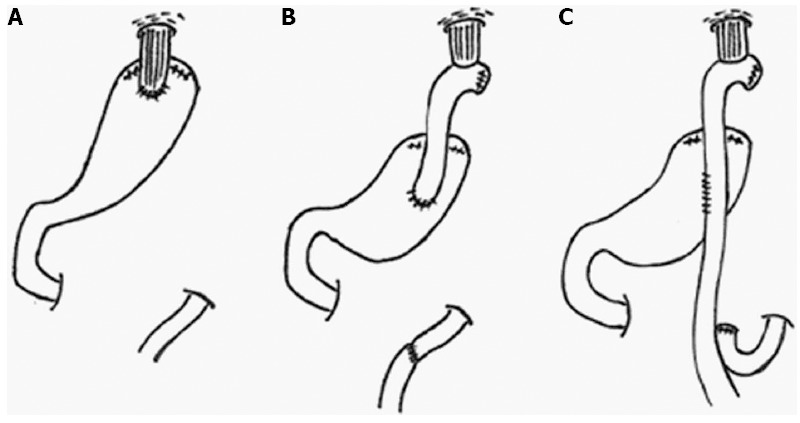
Recent advances in diagnostic techniques have allowed the diagnosis of gastric cancer (GC) at an early stage. Due to the low incidence of lymph node metastasis and favorable prognosis in early GC, function-preserving surgery which improves postoperative quality of life may be possible. Pylorus-preserving gastrectomy (PPG) is one such function-preserving procedure, which is expected to offer advantages with regards to dumping syndrome, bile reflux gastritis, and the frequency of flatus, although PPG may induce delayed gastric emptying. Proximal gastrectomy (PG) is another function-preserving procedure, which is thought to be advantageous in terms of decreased duodenogastric reflux and good food reservoir function in the remnant stomach, although the incidence of heartburn or gastric fullness associated with this procedure is high. However, these disadvantages may be overcome by the reconstruction method used. The other important problem after PG is remnant GC, which was reported to occur in approximately 5% of patients. Therefore, the reconstruction technique used with PG should facilitate postoperative endoscopic examinations for early detection and treatment of remnant gastric carcinoma. Oncologic safety seems to be assured in both procedures, if the preoperative diagnosis is accurate. Patient selection should be carefully considered. Although many retrospective studies have demonstrated the utility of function-preserving surgery, no consensus on whether to adopt function-preserving surgery as the standard of care has been reached. Further prospective randomized controlled trials are necessary to evaluate survival and postoperative quality of life associated with function-preserving surgery.
Keywords: Function preserving surgery; Gastric cancer; Proximal gastrectomy; Pylorus preserving surgery; Quality of life.
Figures
References
-
- Sano T, Hollowood A. Early gastric cancer: diagnosis and less invasive treatments. Scand J Surg. 2006;95:249–255. - PubMed
-
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3) Gastric Cancer. 2011;14:113–123. - PubMed
-
- Maki T, Shiratori T, Hatafuku T, Sugawara K. Pylorus-preserving gastrectomy as an improved operation for gastric ulcer. Surgery. 1967;61:838–845. - PubMed
-
- Sawai K, Takahashi T, Suzuki H. New trends in surgery for gastric cancer in Japan. J Surg Oncol. 1994;56:221–226. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
