

Functional outcome and satisfaction with a "self-care" protocol for the management of mallet finger injuries: a case-series
- PMID: 25516768
- PMCID: PMC4266946
- DOI: 10.1186/s13032-014-0021-y
Functional outcome and satisfaction with a "self-care" protocol for the management of mallet finger injuries: a case-series
Abstract
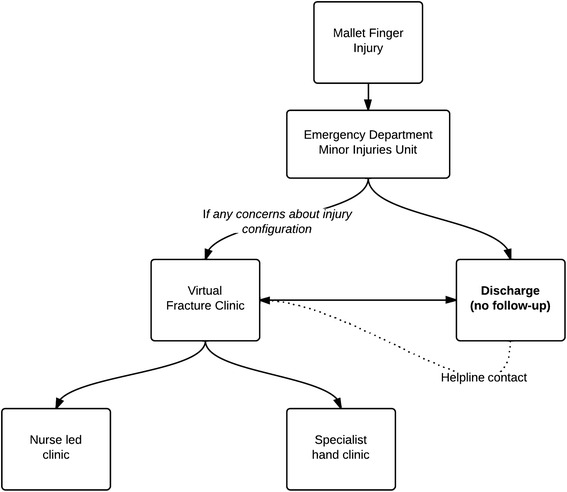
Background: Mallet finger injuries are usually successfully treated non-operatively with a splint. Most patients are reviewed at least twice in a clinic after the initial presentation in A&E. A new protocol promoting "self-care" was introduced at our institution. Patients were provided with structured verbal and written information, and given access to a telephone helpline.
Methods: A prospective electronic patient record was used to identify all patients who presented to the emergency department with a mallet finger with a minimum six month follow-up. A satisfaction and patient reported outcome measure was administered via a postal questionnaire. The response rate was 36/47 (77%).
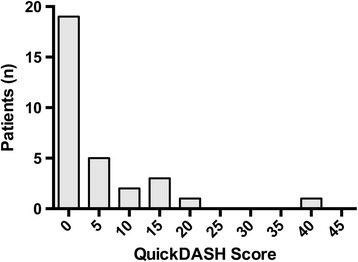
Results: The median QuickDASH score was 2.3 (IQR 0 to 4.6). All patients were satisfied with the treatment plan provided. Nine used the helpline and all were satisfied with information given. Although 13 patients reported some extensor lag, or bump, they had no functional limitation. Seven patients were reviewed by the general practitioner or other clinicians during their treatment period for issues such a skin care, splint size changes or sickness certification. Five were subsequently reviewed at the end of their treatment period in a clinic at their request, or their general practitioner, but did not require further surgical intervention.
Conclusions: Self-care for mallet finger injuries, with adequate patient information and telephone back-up, leads to acceptable functional results and satisfaction.
Level of evidence: III.
Keywords: Extensor tendon; Fracture clinic redesign; Mallet finger; Self-care; Service redesign.
Figures

References
-
- Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg The journal of the American Academy of Psychiatry and the LawJ Am Acad Psychiatry. 2005;13:336–344. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
