

Recent changes in therapeutic approaches and association with outcomes among patients with secondary hyperparathyroidism on chronic hemodialysis: the DOPPS study
- PMID: 25516917
- PMCID: PMC4284424
- DOI: 10.2215/CJN.12941213
Recent changes in therapeutic approaches and association with outcomes among patients with secondary hyperparathyroidism on chronic hemodialysis: the DOPPS study
Abstract
Background and objectives: Elevated parathyroid hormone levels may be associated with adverse clinical outcomes in patients on dialysis. After the introduction of practice guidelines suggesting higher parathyroid hormone targets than those previously recommended, changes in parathyroid hormone levels and treatment regimens over time have not been well documented.
Design, setting, participants, & measurements: Using data from the international Dialysis Outcomes and Practice Patterns Study, trends in parathyroid hormone levels and secondary hyperparathyroidism therapies over the past 15 years and the associations between parathyroid hormone and clinical outcomes are reported; 35,655 participants from the Dialysis Outcomes and Practice Patterns Study phases 1-4 (1996-2011) were included.
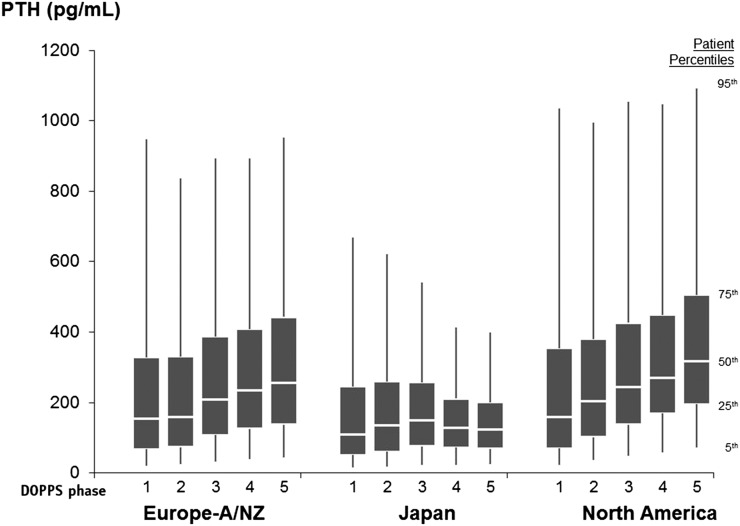
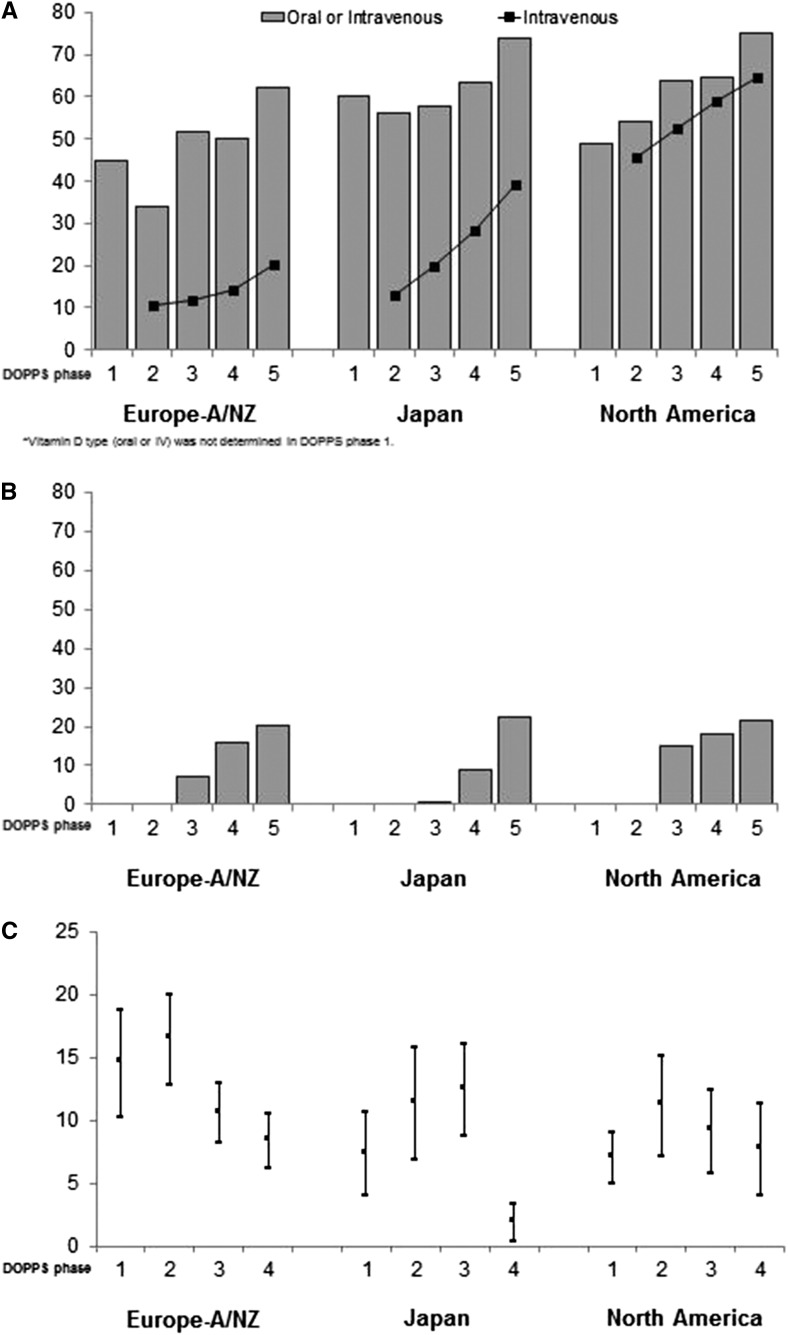
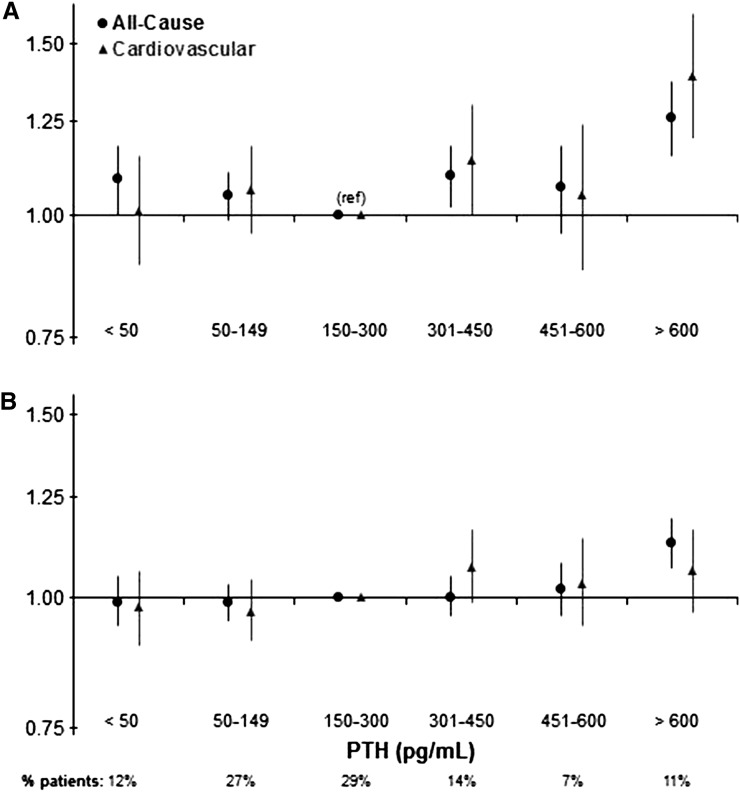
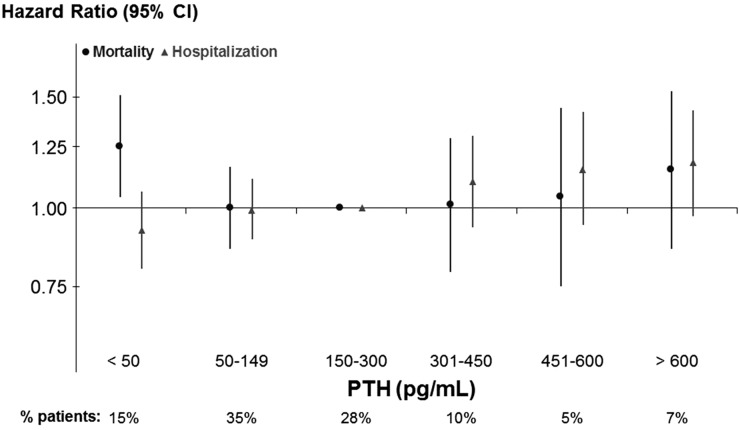
Results: Median parathyroid hormone increased from phase 1 to phase 4 in all regions except for Japan, where it remained stable. Prescriptions of intravenous vitamin D analogs and cinacalcet increased and parathyroidectomy rates decreased in all regions over time. Compared with 150-300 pg/ml, in adjusted models, all-cause mortality risk was higher for parathyroid hormone=301-450 (hazard ratio, 1.09; 95% confidence interval, 1.01 to 1.18) and >600 pg/ml (hazard ratio, 1.23; 95% confidence interval, 1.12 to 1.34). Parathyroid hormone >600 pg/ml was also associated with higher risk of cardiovascular mortality as well as all-cause and cardiovascular hospitalizations. In a subgroup analysis of 5387 patients not receiving vitamin D analogs or cinacalcet and with no prior parathyroidectomy, very low parathyroid hormone (<50 pg/ml) was associated with mortality (hazard ratio, 1.25; 95% confidence interval, 1.04 to 1.51).
Conclusions: In a large international sample of patients on hemodialysis, parathyroid hormone levels increased in most countries, and secondary hyperparathyroidism treatments changed over time. Very low and very high parathyroid hormone levels were associated with adverse outcomes. In the absence of definitive evidence in support of a specific parathyroid hormone target, there is an urgent need for additional research to inform clinical practice.
Keywords: CKD; ESRD; dialysis; hyperparathyroidism; parathyroid hormone.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Dysphoria induced in dialysis providers by secondary hyperparathyroidism.Clin J Am Soc Nephrol. 2015 Jan 7;10(1):9-11. doi: 10.2215/CJN.11551114. Epub 2014 Dec 16. Clin J Am Soc Nephrol. 2015. PMID: 25516914 Free PMC article. No abstract available.
References
-
- United States Renal Data System : 2012 United States Renal Data System Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, 2012 - PubMed
-
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB: Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 342: 1478–1483, 2000 - PubMed
-
- de Francisco AM, Ellis HA, Owen JP, Cassidy MJ, Farndon JR, Ward MK, Kerr DN: Parathyroidectomy in chronic renal failure. Q J Med 55: 289–315, 1985 - PubMed
-
- Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL: Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int 71: 31–38, 2007 - PubMed
-
- Chertow GM, Plone M, Dillon MA, Burke SK, Slatopolsky E: Hyperparathyroidism and dialysis vintage. Clin Nephrol 54: 295–300, 2000 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
