

Increased resource use in lung transplant admissions in the lung allocation score era
- PMID: 25517213
- PMCID: PMC4351576
- DOI: 10.1164/rccm.201408-1562OC
Increased resource use in lung transplant admissions in the lung allocation score era
Abstract
Rationale: In 2005, the lung allocation score (LAS) was implemented to prioritize organ allocation to minimize waiting-list mortality and maximize 1-year survival. It resulted in transplantation of older and sicker patients without changing 1-year survival. Its effect on resource use is unknown.
Objectives: To determine changes in resource use over time in lung transplant admissions.
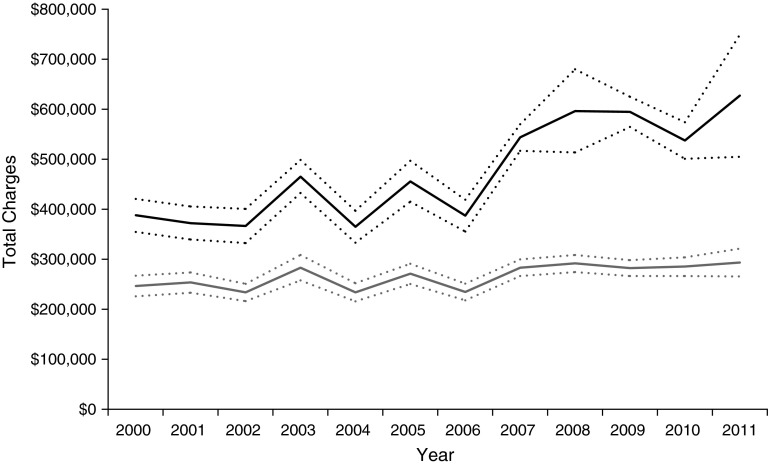
Methods: Solid organ transplant recipients were identified within the Nationwide Inpatient Sample (NIS) data from 2000 to 2011. Joinpoint regression methodology was performed to identify a time point of change in mean total hospital charges among lung transplant and other solid-organ transplant recipients. Two temporal lung transplant recipient cohorts identified by joinpoint regression were compared for baseline characteristics and resource use, including total charges for index hospitalization, charges per day, length of stay, discharge disposition, tracheostomy, and need for extracorporeal membrane oxygenation.
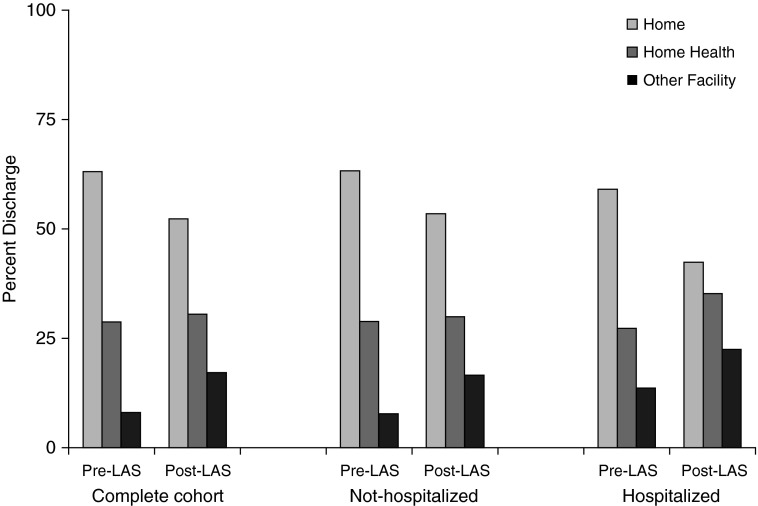
Measurements and main results: A significant point of increased total hospital charges occurred for lung transplant recipients in 2005, corresponding to LAS implementation, which was not seen in other solid-organ transplant recipients. Total transplant hospital charges increased by 40% in the post-LAS cohort ($569,942 [$53,229] vs. $407,489 [$28,360]) along with an increased median length of stay, daily charges, and discharge disposition other than to home. Post-LAS recipients also had higher post-transplant use of extracorporeal membrane oxygenation (odds ratio, 2.35; 95% confidence interval, 1.56-3.55) and higher incidence of tracheostomy (odds ratio, 1.52; 95% confidence interval, 1.22-1.89).
Conclusions: LAS implementation is associated with a significant increase in resource use during index hospitalization for lung transplant.
Keywords: Nationwide Inpatient Sample; lung allocation score; lung transplant; lung transplant cost; solid-organ transplant.
Figures
Comment in
-
Beyond "the LAS is broken". Ways to improve lung allocation.Am J Respir Crit Care Med. 2015 Feb 1;191(3):245-6. doi: 10.1164/rccm.201412-2304ED. Am J Respir Crit Care Med. 2015. PMID: 25635485 No abstract available.
References
-
- Gross CR, Savik K, Bolman RM, III, Hertz MI. Long-term health status and quality of life outcomes of lung transplant recipients. Chest. 1995;108:1587–1593. - PubMed
-
- Yusen RD, Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Dobbels F, Kirk R, Lund LH, Rahmel AO, et al. The registry of the International Society for Heart and Lung Transplantation: Thirtieth Adult Lung and Heart-Lung Transplant Report–2013; focus theme: age. J Heart Lung Transplant. 2013;32:965–978. - PubMed
-
- Egan TM, Murray S, Bustami RT, Shearon TH, McCullough KP, Edwards LB, Coke MA, Garrity ER, Sweet SC, Heiney DA, et al. Development of the new lung allocation system in the United States. Am J Transplantation. 2006;6:1212–1227. - PubMed
-
- Valapour M, Skeans MA, Heubner BM, Smith JM, Schnitzler MA, Hertz MI, Edwards LB, Snyder JJ, Israni AK, Kasiske BL. OPTN/SRTR 2012 annual data report: lung. Am J Transplantation. 2014;14(Suppl. 1):139–165. - PubMed
-
- Lingaraju R, Blumenthal NP, Kotloff RM, Christie J, Ahya VN, Sager JS, Pochettino A, Hadjiliadis D. Effects of lung allocation score on waiting list rankings and transplant procedures. J Heart Lung Transplant. 2006;25:1167–1170. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
