

Recurrent posterior circulation infarction caused by anomalous occipital bony process in a young patient
- PMID: 25519166
- PMCID: PMC4302142
- DOI: 10.1186/s12883-014-0252-6
Recurrent posterior circulation infarction caused by anomalous occipital bony process in a young patient
Abstract
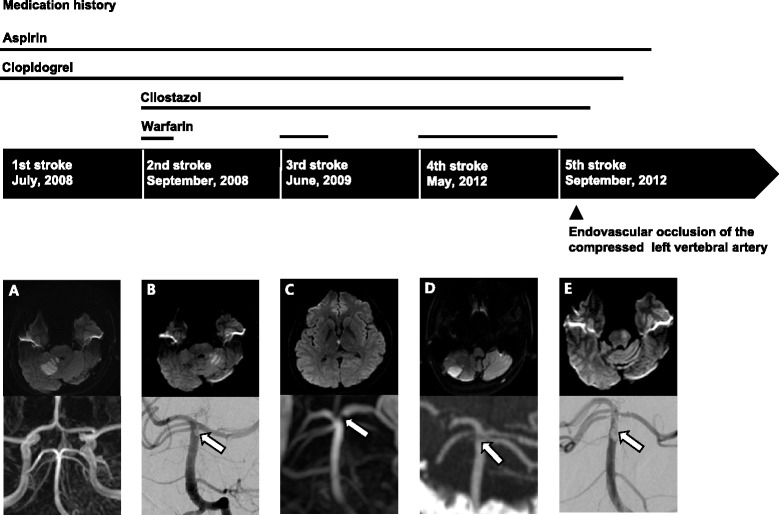
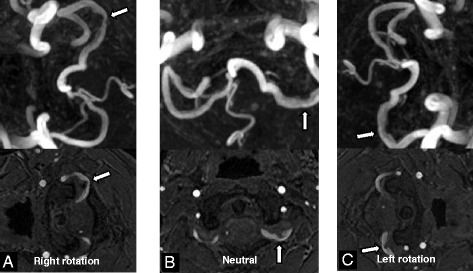
Background: Structural anomaly of the cervical spine or craniocervical junction has been reported as one of the rare causes of ischemic stroke. We report a case of a young patient with recurrent posterior circulation infarction that may have been associated with an anomalous occipital bony process compressing the vertebral artery.
Case presentation: A 23-year-old man experienced recurrent posterior circulation infarction 5 times over a period of 5 years. He had no conventional vascular risk factors. Young age stroke work-up including thorough cardiac, intra- and extracranial vascular evaluation and laboratory tests for the hypercoagulable state or connective tissue disease yielded unremarkable results. An anomalous bony process from the occipital base compressing the left vertebral artery was observed on brain CT. All the recurrent strokes were explainable by the arterial thromboembolism originating from the compressed left vertebral artery. Therefore, the left vertebral artery compressed by the anomalous occipital bony process may have been the culprit behind the recurrent thromboembolic strokes in our patient. Intractable recurrent strokes even under optimal medical treatment led us to make a decision for the intervention. Instead of surgical removal of the anomalous occipital bony process, the left vertebral artery was occluded permanently by endovascular coiling after confirming that this would cause no neurological deficits or flow disturbance in the posterior circulation. There was no recurrence of stroke for 2 years after permanent occlusion of the left vertebral artery.
Conclusion: Arterial thromboembolism originating from the left vertebral artery compressed by the anomalous occipital bony process is a rare but not to be overlooked cause of posterior circulation infarction. When intractable to medical treatment, endovascular occlusion of the vertebral artery without flow disturbance to the posterior circulation may be a useful treatment option when surgical removal is not feasible.
Figures


References
-
- Renna R, Pilato F, Profice P, Della Marca G, Broccolini A, Morosetti R, Frisullo G, Rossi E, De Stefano V, Di Lazzaro V. Risk factor and etiology analysis of ischemic stroke in young adult patients. J Stroke Cerebrovasc Dis. 2014;23:e221–e227. doi: 10.1016/j.jstrokecerebrovasdis.2013.10.008. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
