

Review
doi: 10.3389/fpsyt.2014.00155.
eCollection 2014.
Actigraphy, the alternative way?
Affiliations
- PMID: 25520671
- PMCID: PMC4253804
- DOI: 10.3389/fpsyt.2014.00155
Item in Clipboard
Review
Actigraphy, the alternative way?
Front Psychiatry.
.
No abstract available
Keywords: MSLT; actigraphy; longtime recording; polysomnography; sleep disorders.
Figures
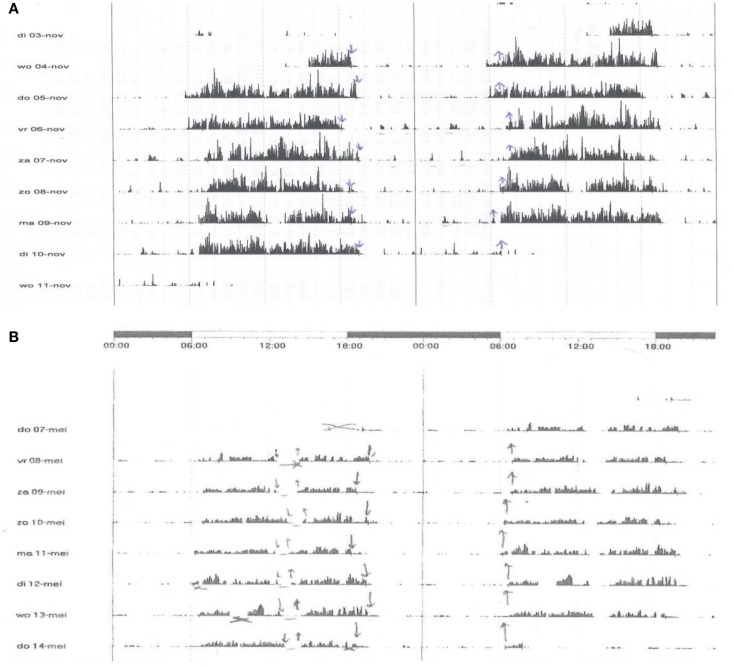
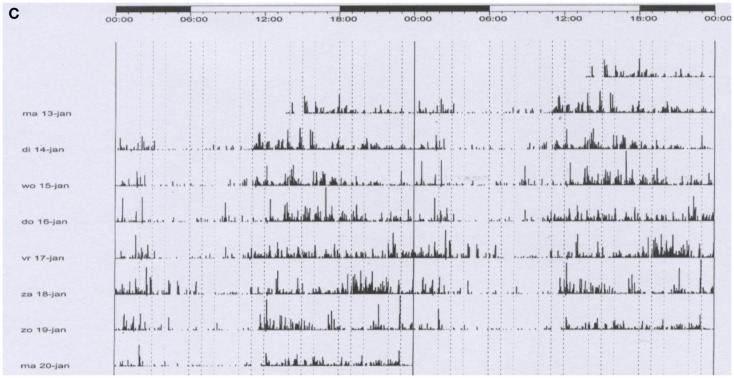
The figure shows three registrations of actigraphy over a period of 7–8 days. Each line represents 48 h. The plots are printed in a cascade mode: the right half of each line is printed as well as the left part of the next line in order to show clearly what happens around midnight. Arrows downward represent the moment of lights off; the upward arrows out of bed. (A) A boy, 3 years old, with insomnia and limit setting disorder. He sleeps from app. 7:30 p.m. to 6:30 a.m. Each night, he is very noisy when awake and terrorizes his parents. The actigraphy shows his regular bedtimes and the distinct periods of being active. Cognitive and behavioral therapy, in particular strict negation of the events during the night, was given to parents and child with good success. (B) A girl, 12 years old, complained about insomnia and tiredness during daytime. She felt sleepy in the afternoon. Actigraphy shows a prolonged sleep time of app. 12 h (7:00 p.m. to 7:00 a.m.) and regular naps after lunch. The differential diagnosis was long sleeper hypersomnia, bad sleep hygiene, or both. Narcolepsy was not expected due to lack of other phenomena, such as cataplexy and hallucinations. Polysomnography showed many spontaneous arousals and short awakenings. The main diagnosis was bad sleep hygiene. Cognitive and behavioral therapy resulted in a sleep period of app. 10 h when measured over the full 24 h. Sleep quality improved as did the tiredness. Naps were no longer necessary. This example shows as well that actigraphy has face value for the assessment of hypersomnia. (C) A boy 14 years of age. He ca not sleep before 2 o’clock in the morning and has severe problems to come out of bed before 11 a.m. Obviously, he fails at school, in particular in the first hours of morning classes. Actigraphy shows the real sleep/wake pattern. The diagnosis is Delayed Sleep Phase Syndrome. Cognitive and behavioral therapy, endorsed by light therapy, led to a satisfactory situation with timing of sleep between 11.30 p.m. and 8.15 a.m. This example shows the important role of actigraphy in the assessment of disturbances of the biological clock.
The figure shows three registrations of actigraphy over a period of 7–8 days. Each line represents 48 h. The plots are printed in a cascade mode: the right half of each line is printed as well as the left part of the next line in order to show clearly what happens around midnight. Arrows downward represent the moment of lights off; the upward arrows out of bed. (A) A boy, 3 years old, with insomnia and limit setting disorder. He sleeps from app. 7:30 p.m. to 6:30 a.m. Each night, he is very noisy when awake and terrorizes his parents. The actigraphy shows his regular bedtimes and the distinct periods of being active. Cognitive and behavioral therapy, in particular strict negation of the events during the night, was given to parents and child with good success. (B) A girl, 12 years old, complained about insomnia and tiredness during daytime. She felt sleepy in the afternoon. Actigraphy shows a prolonged sleep time of app. 12 h (7:00 p.m. to 7:00 a.m.) and regular naps after lunch. The differential diagnosis was long sleeper hypersomnia, bad sleep hygiene, or both. Narcolepsy was not expected due to lack of other phenomena, such as cataplexy and hallucinations. Polysomnography showed many spontaneous arousals and short awakenings. The main diagnosis was bad sleep hygiene. Cognitive and behavioral therapy resulted in a sleep period of app. 10 h when measured over the full 24 h. Sleep quality improved as did the tiredness. Naps were no longer necessary. This example shows as well that actigraphy has face value for the assessment of hypersomnia. (C) A boy 14 years of age. He ca not sleep before 2 o’clock in the morning and has severe problems to come out of bed before 11 a.m. Obviously, he fails at school, in particular in the first hours of morning classes. Actigraphy shows the real sleep/wake pattern. The diagnosis is Delayed Sleep Phase Syndrome. Cognitive and behavioral therapy, endorsed by light therapy, led to a satisfactory situation with timing of sleep between 11.30 p.m. and 8.15 a.m. This example shows the important role of actigraphy in the assessment of disturbances of the biological clock.
References
-
- Sadeh A. Actigraphy. In: Guilleminault C, editor. Clinical Neurophysiology of Sleep Disorders Handbook of Clinical Neurophysiology Series. Vol. 6, Philadelphia: Elsevier/Saunders; (2005). p. 67–72.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources