

Age-associated white matter lesions: the MRC Cognitive Function and Ageing Study
- PMID: 25521175
- PMCID: PMC8029351
- DOI: 10.1111/bpa.12219
Age-associated white matter lesions: the MRC Cognitive Function and Ageing Study
Abstract
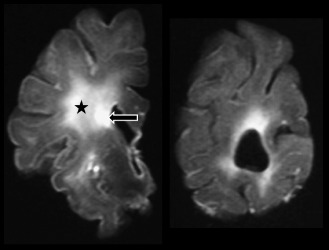
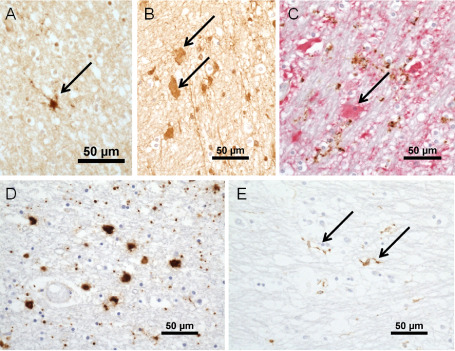
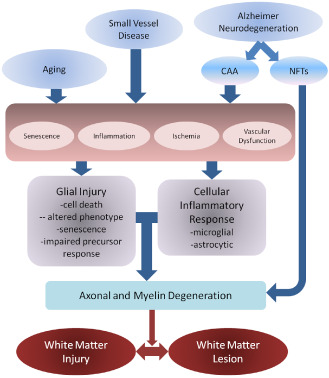
Cerebral white matter lesions (WML) are common in the aging brain and are associated with dementia and depression. They are associated with vascular risk factors and small vessel disease, suggesting an ischemic origin, but recent pathology studies suggest a more complex pathogenesis. Studies using samples from the population-representative Medical Research Council Cognitive Function and Ageing Study neuropathology cohort used post-mortem magnetic resonance imaging to identify WML for further study. Expression of hypoxia-related molecules and other injury and protective cellular pathways in candidate immunohistochemical and gene expression microarray studies support a role for hypoxia/ischemia. However, these approaches also suggest that immune activation, blood-brain barrier dysfunction, altered cell metabolic pathways and glial cell injury contribute to pathogenesis. These abnormalities are not confined to WML, but are also found in apparently normal white matter in brains with lesions, suggesting a field effect of white matter abnormality within which lesions arise. WML are an active pathology with a complex pathogenesis that may potentially offer a number of primary and secondary intervention targets.
Keywords: aging; blood-brain barrier; dementia; small vessel disease; vascular; white matter lesions.
© 2014 International Society of Neuropathology.
Figures
References
-
- Akiguchi I, Tomimoto H, Suenaga T, Wakita H, Budka H (1997) Alterations in glia and axons in the brains of Binswangers disease patients. Stroke 28:1423–1429. - PubMed
-
- Bakker S, de Leeuw F, de Groot C, Hofman A, Koudstaal P, Breteler M (1999) Cerebral vasomotor reactivity and cerebral white matter lesions in the elderly. Neurology 52:578–583. - PubMed
-
- Boche D, Perry V, Nicoll J (2013) Activation patterns of microglia and their identification in the human brain. Neuropathol Appl Neurobiol 39:3–18. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
