

Simvastatin prevents and reverses depigmentation in a mouse model of vitiligo
- PMID: 25521459
- PMCID: PMC4366328
- DOI: 10.1038/jid.2014.529
Simvastatin prevents and reverses depigmentation in a mouse model of vitiligo
Abstract
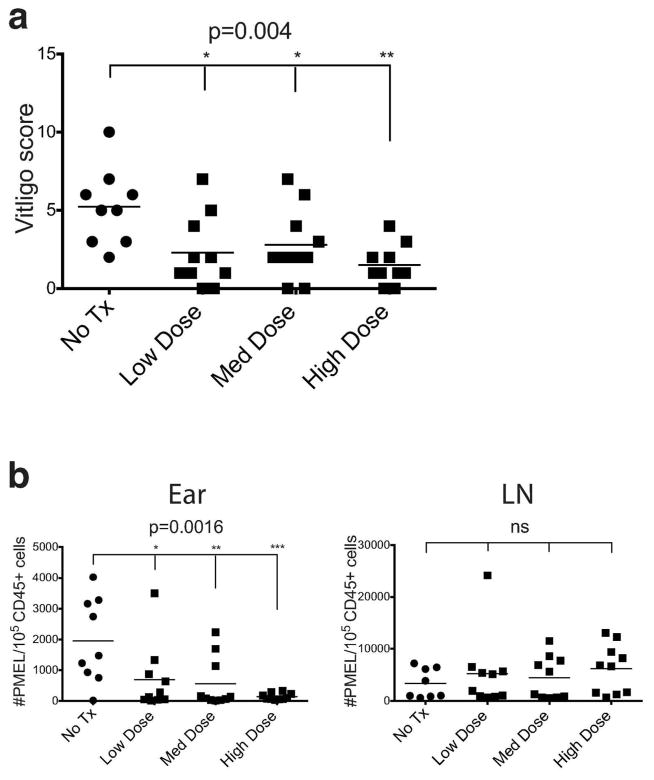
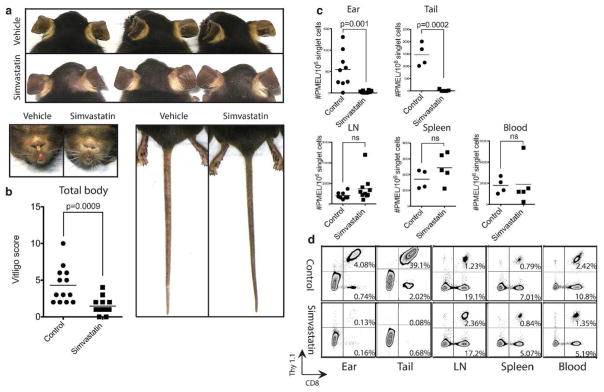
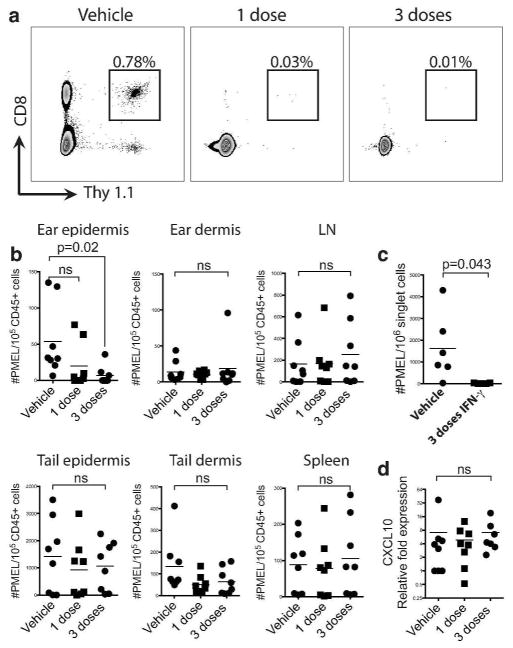
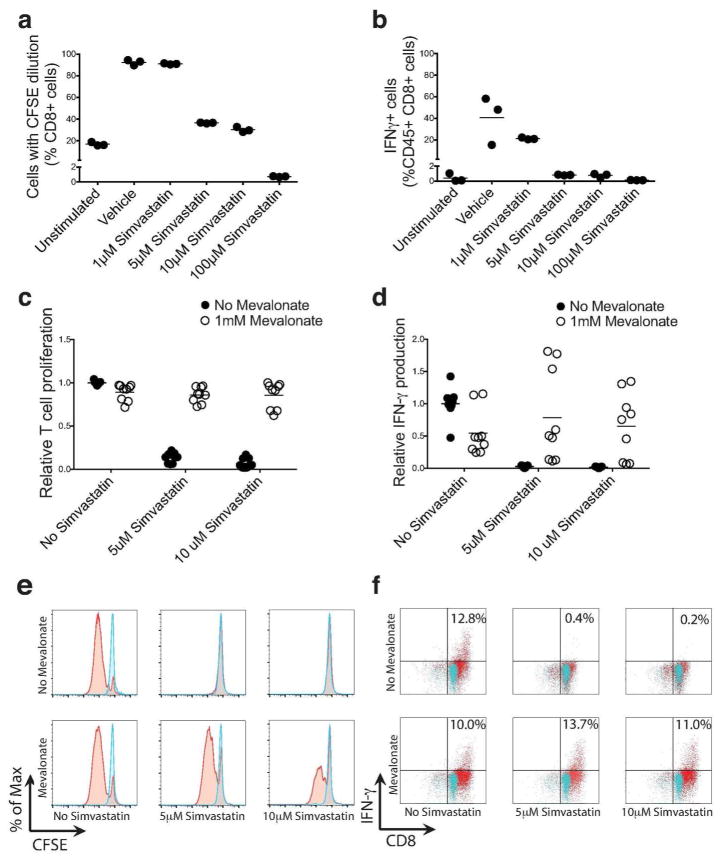
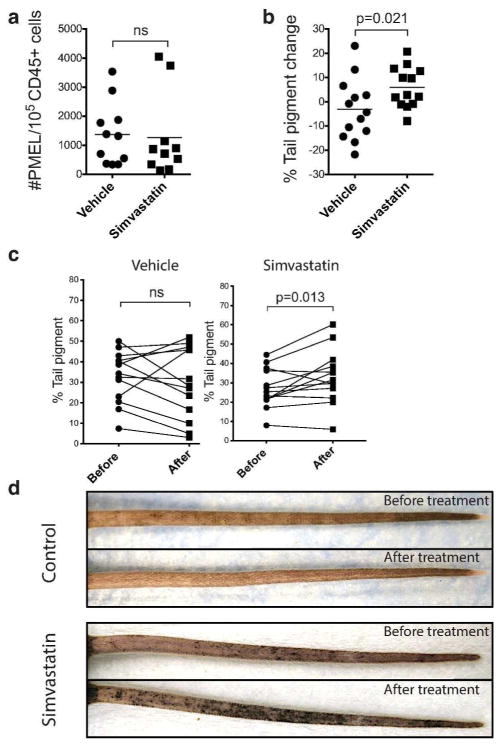
Vitiligo is a common autoimmune disease of the skin that results in disfiguring white spots. There are no Food and Drug Administration (FDA)-approved treatments, and current treatments are time-consuming, expensive, and of low efficacy. We sought to identify new treatments for vitiligo, and first considered repurposed medications because of the availability of safety data and expedited regulatory approval. We previously reported that the IFN-γ-induced chemokine CXCL10 is expressed in lesional skin from vitiligo patients, and that it is critical for the progression and maintenance of depigmentation in our mouse model of vitiligo. We hypothesized that targeting IFN-γ signaling might be an effective new treatment strategy. Activation of signal transducer and activator of transcription 1 (STAT1) is required for IFN-γ signaling and recent studies revealed that simvastatin, an FDA-approved cholesterol-lowering medication, inhibited STAT1 activation in vitro. Therefore, we hypothesized that simvastatin may be an effective treatment for vitiligo. We found that simvastatin both prevented and reversed depigmentation in our mouse model of vitiligo, and reduced the number of infiltrating autoreactive CD8(+) T cells in the skin. Treatment of melanocyte-specific, CD8(+) T cells in vitro decreased proliferation and IFN-γ production, suggesting additional effects of simvastatin directly on T cells. Based on these data, simvastatin may be a safe, targeted treatment option for patients with vitiligo.
Conflict of interest statement
The authors state no conflict of interest.
Figures
References
-
- Aaronson DS, Horvath CM. A road map for those who don’t know JAK-STAT. Science. 2002;296:1653–5. - PubMed
-
- Alghamdi KM, Khurrum H, Rikabi A. Worsening of vitiligo and onset of new psoriasiform dermatitis following treatment with infliximab. Journal of cutaneous medicine and surgery. 2011;15:280–4. - PubMed
-
- Alghamdi KM, Khurrum H, Taieb A, et al. Treatment of generalized vitiligo with anti-TNF-alpha Agents. J Drugs Dermatol. 2012;11:534–9. - PubMed
-
- Alikhan A, Felsten LM, Daly M, et al. Vitiligo: a comprehensive overview Part I. Introduction, epidemiology, quality of life, diagnosis, differential diagnosis, associations, histopathology, etiology, and work-up. J Am Acad Dermatol. 2011;65:473–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
