

Outcomes of extremely preterm infants after delivery room cardiopulmonary resuscitation in a population-based cohort
- PMID: 25521563
- PMCID: PMC4414658
- DOI: 10.1038/jp.2014.222
Outcomes of extremely preterm infants after delivery room cardiopulmonary resuscitation in a population-based cohort
Abstract
Objective: To describe the relationship of delivery room cardiopulmonary resuscitation (DR-CPR) to short-term outcomes of extremely preterm infants.
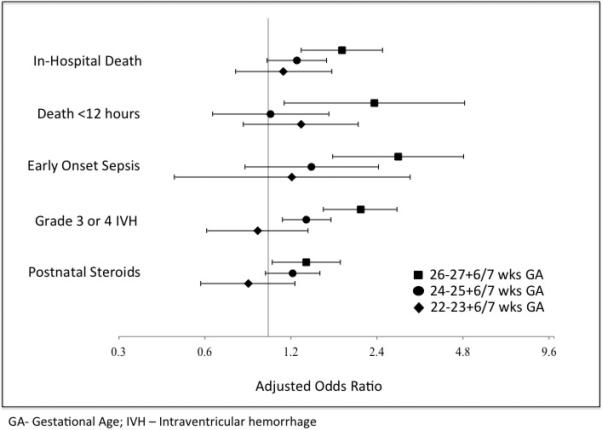
Study design: This was a cohort study of 22 to 27+6/7 weeks gestational age (GA) infants during 2005 to 2011. DR-CPR was defined as chest compressions and/or epinephrine administration. Multivariable logistic regression was used to estimate odds ratios (ORs) with 95% confidence intervals (CIs) associated with DR-CPR; analysis was stratified by GA.
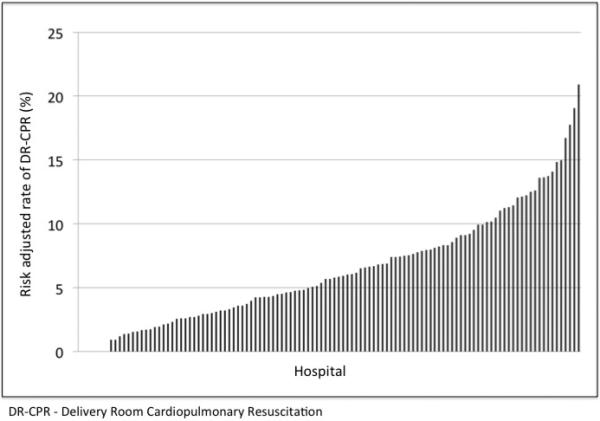
Result: Of the 13 758 infants, 856 (6.2%) received DR-CPR. Infants 22 to 23+6/7 weeks receiving DR-CPR had similar outcomes to non-recipients. Infants 24 to 25+6/7 weeks receiving DR-CPR had more severe intraventricular hemorrhage (OR 1.36, 95% CI 1.07, 1.72). Infants 26 to 27+6/7 weeks receiving DR-CPR were more likely to die (OR 1.81, 95% CI 1.30, 2.51) and have intraventricular hemorrhage (OR 2.10, 95% CI 1.56, 2.82). Adjusted hospital DR-CPR rates varied widely (median 5.7%).
Conclusion: Premature infants receiving DR-CPR had worse outcomes. Mortality and morbidity varied by GA.
Figures
References
-
- Hack M, Friedman H, Fanaroff AA. Outcomes of extremely low birth weight infants. Pediatrics. 1996;98(5):931–937. - PubMed
-
- Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ, et al. Very low birth weight outcomes of the National Institute of Child health and human development neonatal research network, January 1995 through December 1996. NICHD Neonatal Research Network. Pediatrics. 2001;107(1):E1. - PubMed
-
- Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR, et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196(2):147, e141–148. - PubMed
-
- Hintz SR, Kendrick DE, Vohr BR, Poole WK, Higgins RD. Changes in neurodevelopmental outcomes at 18 to 22 months' corrected age among infants of less than 25 weeks' gestational age born in 1993-1999. Pediatrics. 2005;115(6):1645–1651. - PubMed
-
- Horbar JD, Badger GJ, Carpenter JH, Fanaroff AA, Kilpatrick S, LaCorte M, et al. Trends in mortality and morbidity for very low birth weight infants, 1991-1999. Pediatrics. 2002;110(1 Pt 1):143–151. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
