

CT features of pulmonary arterial hypertension and its major subtypes: a systematic CT evaluation of 292 patients from the ASPIRE Registry
- PMID: 25523307
- PMCID: PMC4392204
- DOI: 10.1136/thoraxjnl-2014-206088
CT features of pulmonary arterial hypertension and its major subtypes: a systematic CT evaluation of 292 patients from the ASPIRE Registry
Abstract
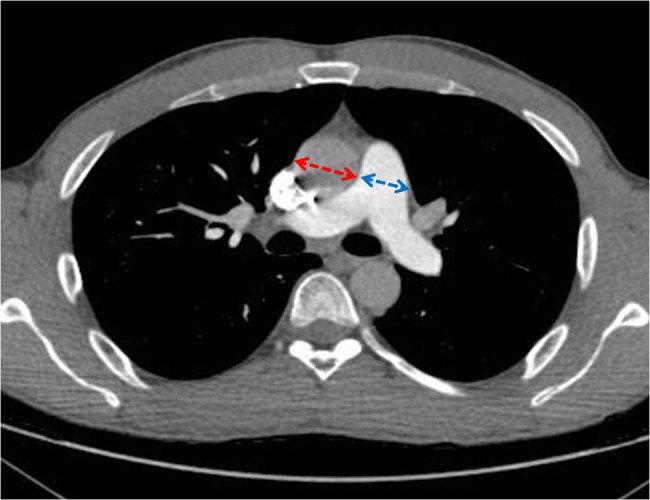
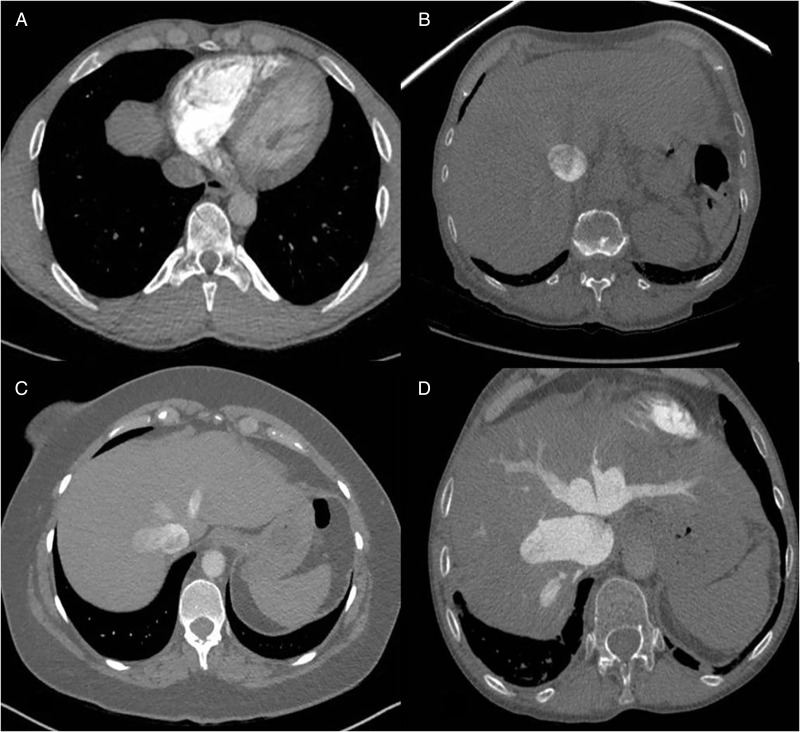
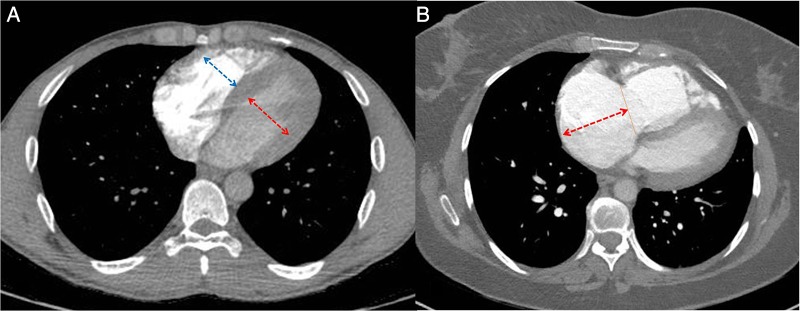
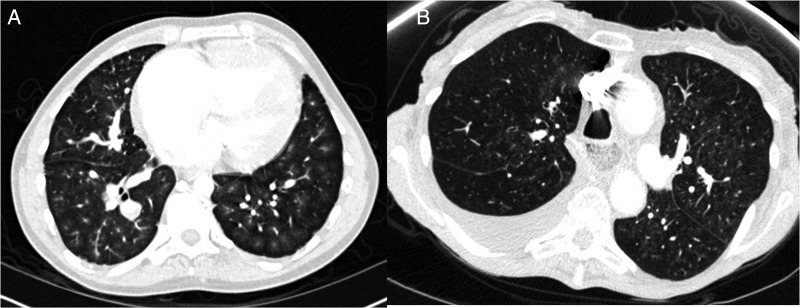
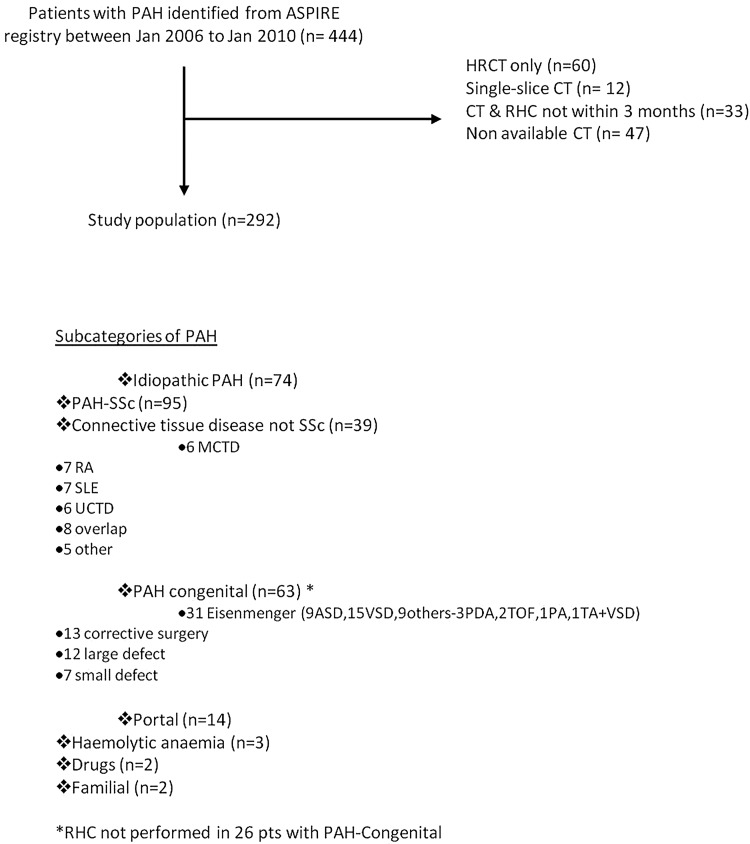
We evaluated the prevalence and prognostic value of CT-pulmonary angiographic (CTPA) measures in 292 treatment naive patients with pulmonary arterial hypertension (PAH). Pulmonary artery calcification (13%) and thrombus (10%) were exclusively seen in PAH-congenital heart disease. Oesophageal dilation (46%) was most frequent in PAH-systemic sclerosis. Ground glass opacification (GGO) (41%), pericardial effusion (38%), lymphadenopathy (19%) and pleural effusion (11%) were common. On multivariate analysis, inferior vena caval area, the presence of pleural effusion and septal lines predicted outcome. In PAH, CTPA provides diagnostic and prognostic information. In addition, the presence of GGO on a CT performed for unexplained breathlessness should alert the physician to the possibility of PAH.
Keywords: Primary Pulmonary Hypertension.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

Comment in
-
Incremental value of pulmonary artery diameter indexed for BSA in pulmonary hypertension.Thorax. 2015 Nov;70(11):1087. doi: 10.1136/thoraxjnl-2015-207328. Epub 2015 Jun 23. Thorax. 2015. PMID: 26103994 No abstract available.
-
Response to: 'CT assessment for pulmonary hypertension requires systematic assessment of cardiac, vascular and parenchymal signs' by Marloes et al.Thorax. 2015 Nov;70(11):1087-8. doi: 10.1136/thoraxjnl-2015-207394. Epub 2015 Jun 24. Thorax. 2015. PMID: 26108572 No abstract available.
References
-
- Hurdman J, Condliffe R, Elliot CA, et al. Aspire Registry: assessing the spectrum of pulmonary hypertension identified at a referral centre. Eur Respir J 2012;39:945–55. - PubMed
-
- Nagueh SF, Kopelen HA, Zoghbi WA. Relation of mean right atrial pressure to echocardiographic and Doppler parameters of right atrial and right ventricular function. Circulation 1996;93:1160–9. - PubMed
-
- Sherrick AD, Swensen SJ, Hartman TE. Mosaic pattern of lung attenuation on CT scans: frequency among patients with pulmonary artery hypertension of different causes. AJR Am J Roentgenol 1997;169:79–82. - PubMed
-
- Resten A, Maitre S, Humbert M, et al. Pulmonary arterial hypertension: thin-section CT predictors of epoprostenol therapy failure. Radiology 2002;222:782–8. - PubMed
-
- Resten A, Maitre S, Humbert M, et al. Pulmonary hypertension: CT of the chest in pulmonary venoocclusive disease. AJR Am J Roentgenol 2004;183:65–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical