

Clinical phenotype and outcome of hypertrophic cardiomyopathy associated with thin-filament gene mutations
- PMID: 25524337
- PMCID: PMC4270453
- DOI: 10.1016/j.jacc.2014.09.059
Clinical phenotype and outcome of hypertrophic cardiomyopathy associated with thin-filament gene mutations
Abstract
Background: Mild hypertrophy but increased arrhythmic risk characterizes the stereotypic phenotype proposed for hypertrophic cardiomyopathy (HCM) caused by thin-filament mutations. However, whether such clinical profile is different from more prevalent thick-filament-associated disease is unresolved.
Objectives: This study aimed to assess clinical features and outcomes in a large cohort of patients with HCM associated with thin-filament mutations compared with thick-filament HCM.
Methods: Adult HCM patients (age >18 years), 80 with thin-filament and 150 with thick-filament mutations, were followed for an average of 4.5 years.
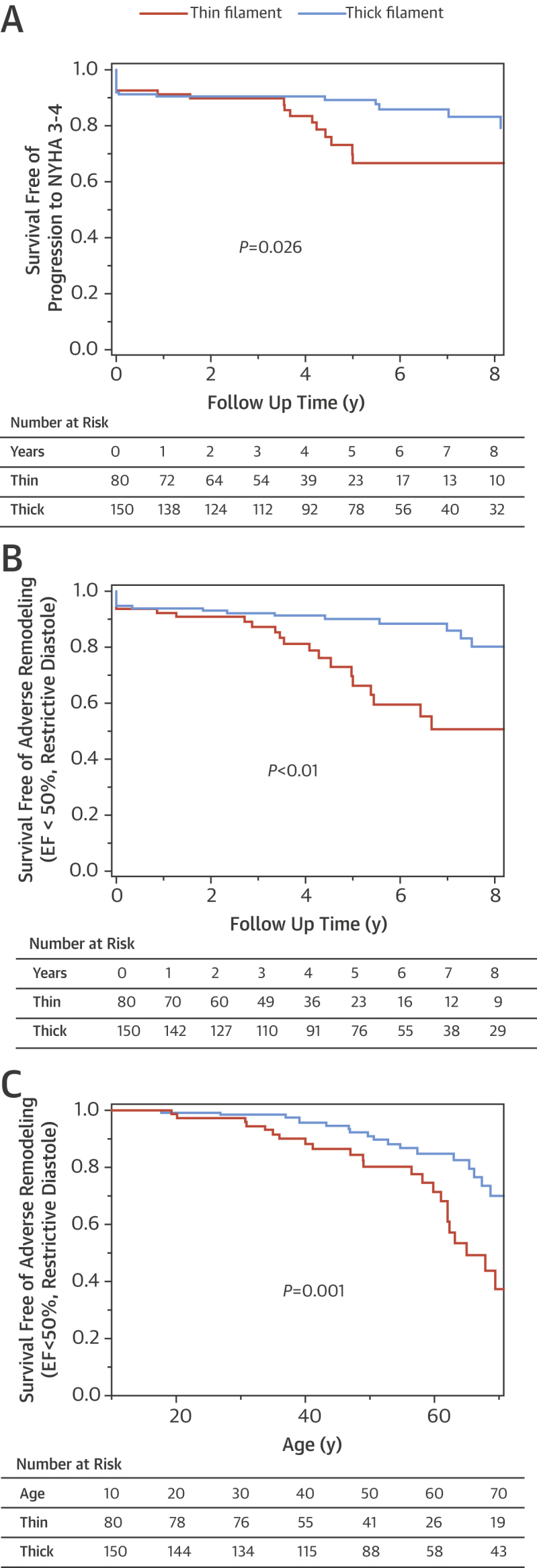
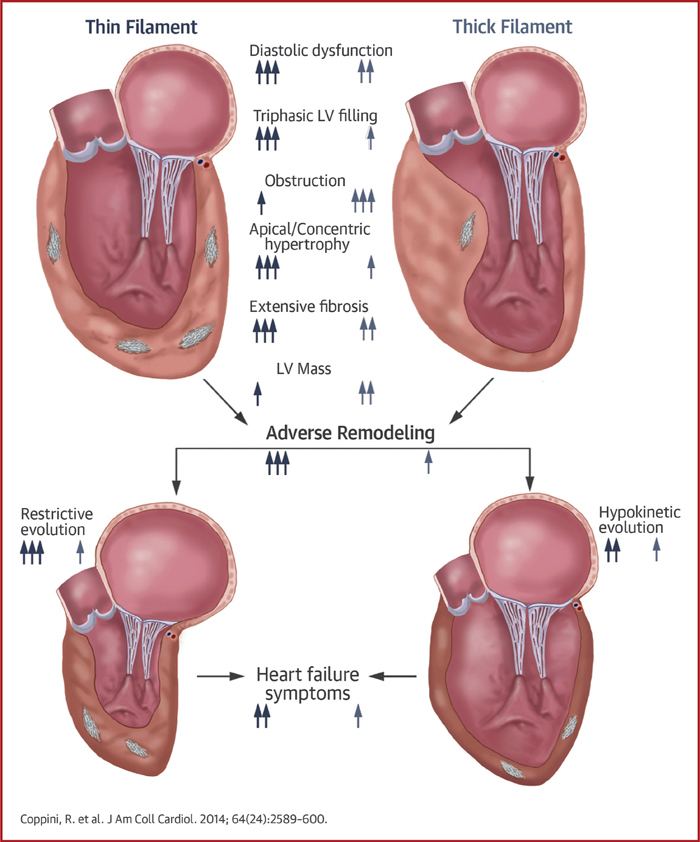
Results: Compared with thick-filament HCM, patients with thin-filament mutations showed: 1) milder and atypically distributed left ventricular (LV) hypertrophy (maximal wall thickness 18 ± 5 mm vs. 24 ± 6 mm; p < 0.001) and less prevalent outflow tract obstruction (19% vs. 34%; p = 0.015); 2) higher rate of progression to New York Heart Association functional class III or IV (15% vs. 5%; p = 0.013); 3) higher prevalence of systolic dysfunction or restrictive LV filling at last evaluation (20% vs. 9%; p = 0.038); 4) 2.4-fold increase in prevalence of triphasic LV filling pattern (26% vs. 11%; p = 0.002); and 5) similar rates of malignant ventricular arrhythmias and sudden cardiac death (p = 0.593).
Conclusions: In adult HCM patients, thin-filament mutations are associated with increased likelihood of advanced LV dysfunction and heart failure compared with thick-filament disease, whereas arrhythmic risk in both subsets is comparable. Triphasic LV filling is particularly common in thin-filament HCM, reflecting profound diastolic dysfunction.
Keywords: diastolic function; end-stage; genotype to phenotype correlation; triphasic filling; troponin.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Thin-filament mutations, hypertrophic cardiomyopathy, and risk.J Am Coll Cardiol. 2014 Dec 23;64(24):2601-2604. doi: 10.1016/j.jacc.2014.10.007. J Am Coll Cardiol. 2014. PMID: 25524338 No abstract available.
References
-
- Maron B.J., Maron M.S., Semsarian C. Genetics of hypertrophic cardiomyopathy after 20 years: clinical perspectives. J Am Coll Cardiol. 2012;60:705–715. - PubMed
-
- Olivotto I., Girolami F., Ackerman M.J., et al. Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin Proc. 2008;83:630–638. - PubMed
-
- Thierfelder L., Watkins H., MacRae C., et al. Alpha-tropomyosin and cardiac troponin T mutations cause familial hypertrophic cardiomyopathy: a disease of the sarcomere. Cell. 1994;77:701–712. - PubMed
-
- Van Driest S.L., Ellsworth E.G., Ommen S.R., Tajik A.J., Gersh B.J., Ackerman M.J. Prevalence and spectrum of thin filament mutations in an outpatient referral population with hypertrophic cardiomyopathy. Circulation. 2003;108:445–451. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
