

Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings
- PMID: 25524718
- PMCID: PMC4528347
- DOI: 10.1186/1472-6882-14-511
Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings
Abstract
Background: Polycystic ovary syndrome (PCOS) is a prevalent, complex endocrine disorder characterised by polycystic ovaries, chronic anovulation and hyperandrogenism leading to symptoms of irregular menstrual cycles, hirsutism, acne and infertility. Evidence based medical management emphasises a multidisciplinary approach for PCOS, as conventional pharmaceutical treatment addresses single symptoms, may be contra-indicated, is often associated with side effects and not effective in some cases. In addition women with PCOS have expressed a strong desire for alternative treatments. This review examines the reproductive endocrine effects in PCOS for an alternative treatment, herbal medicine. The aim of this review was to identify consistent evidence from both pre-clinical and clinical research, to add to the evidence base for herbal medicine in PCOS (and associated oligo/amenorrhoea and hyperandrogenism) and to inform herbal selection in the provision clinical care for these common conditions.
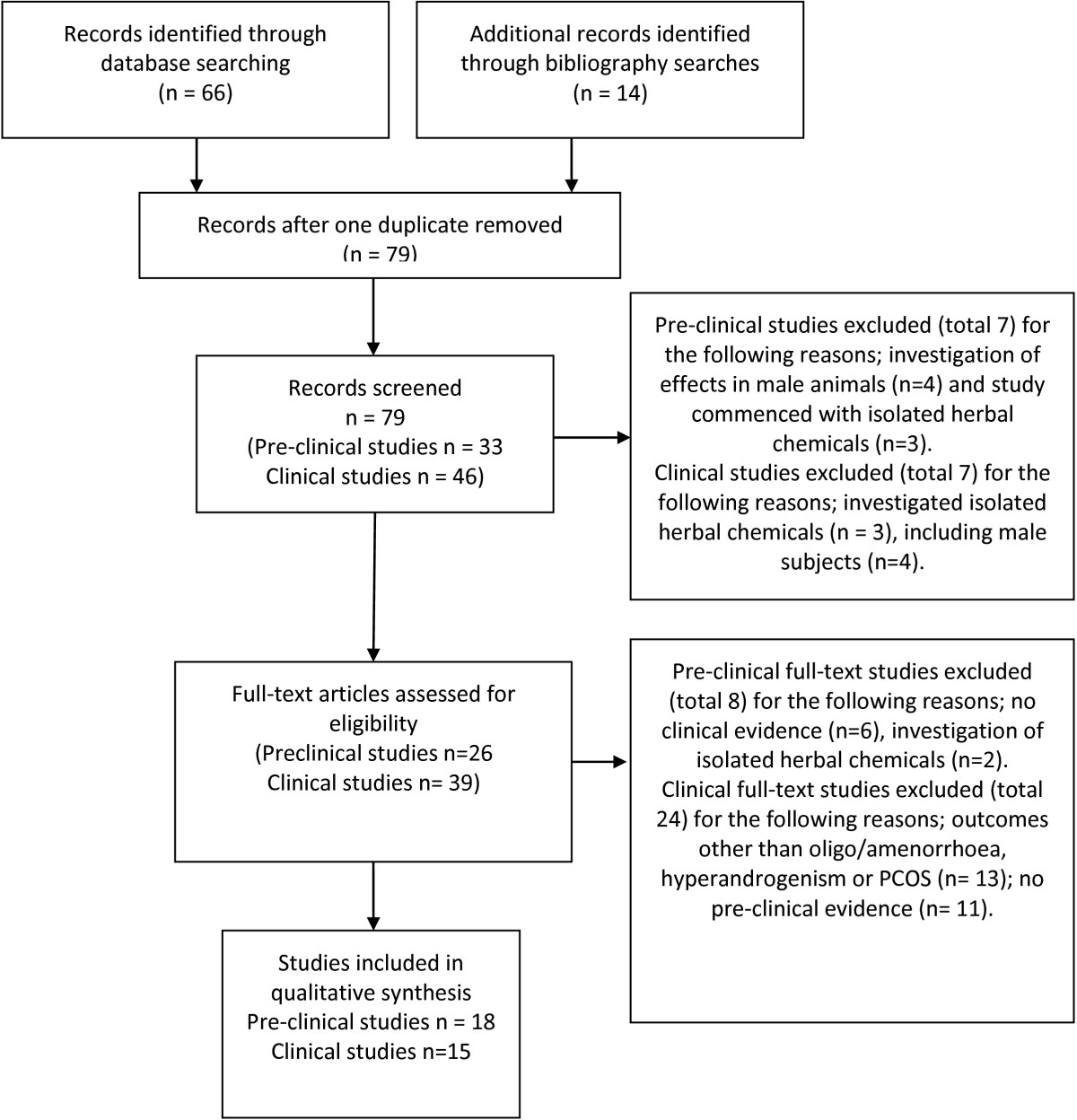
Methods: We undertook two searches of the scientific literature. The first search sought pre-clinical studies which explained the reproductive endocrine effects of whole herbal extracts in oligo/amenorrhoea, hyperandrogenism and PCOS. Herbal medicines from the first search informed key words for the second search. The second search sought clinical studies, which corroborated laboratory findings. Subjects included women with PCOS, menstrual irregularities and hyperandrogenism.
Results: A total of 33 studies were included in this review. Eighteen pre-clinical studies reported mechanisms of effect and fifteen clinical studies corroborated pre-clinical findings, including eight randomised controlled trials, and 762 women with menstrual irregularities, hyperandrogenism and/or PCOS. Interventions included herbal extracts of Vitex agnus-castus, Cimicifuga racemosa, Tribulus terrestris, Glycyrrhiza spp., Paeonia lactiflora and Cinnamomum cassia. Endocrine outcomes included reduced luteinising hormone (LH), prolactin, fasting insulin and testosterone. There was evidence for the regulation of ovulation, improved metabolic hormone profile and improved fertility outcomes in PCOS. There was evidence for an equivalent effect of two herbal medicines and the pharmaceutical agents bromocriptine (and Vitex agnus-castus) and clomiphene citrate (and Cimicifuga racemosa). There was less robust evidence for the complementary combination of spirinolactone and Glycyrrhiza spp. for hyperandrogenism.
Conclusions: Preclinical and clinical studies provide evidence that six herbal medicines may have beneficial effects for women with oligo/amenorrhea, hyperandrogenism and PCOS. However the quantity of pre-clinical data was limited, and the quality of clinical evidence was variable. Further pre-clinical studies are needed to explain the effects of herbal medicines not included in this review with current clinical evidence but an absence of pre-clinical data.
Figures
References
-
- Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2010;1:2–12. - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6882/14/511/prepub
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
