

Prognostic factors for remission of and survival in acquired hemophilia A (AHA): results from the GTH-AH 01/2010 study
- PMID: 25525118
- PMCID: PMC4326770
- DOI: 10.1182/blood-2014-07-587089
Prognostic factors for remission of and survival in acquired hemophilia A (AHA): results from the GTH-AH 01/2010 study
Abstract
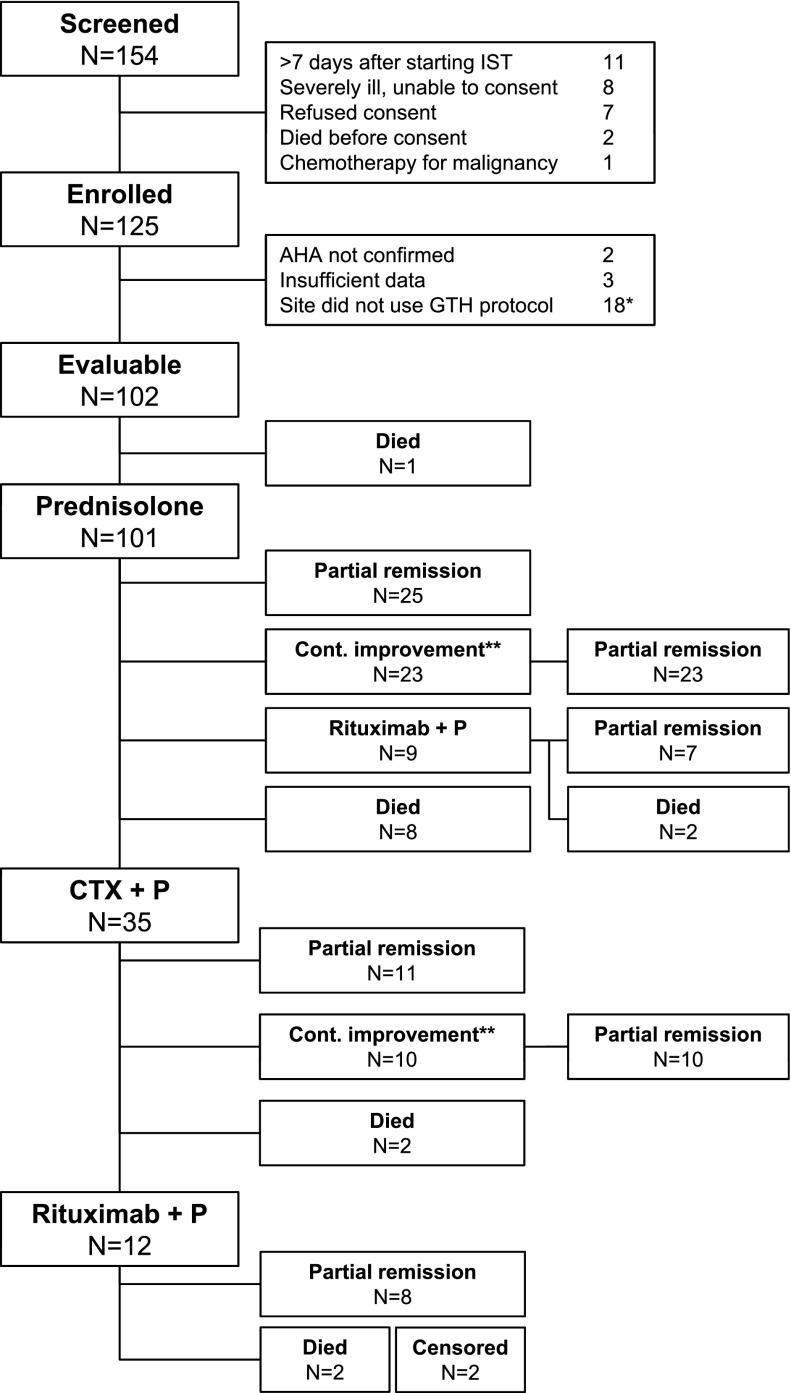
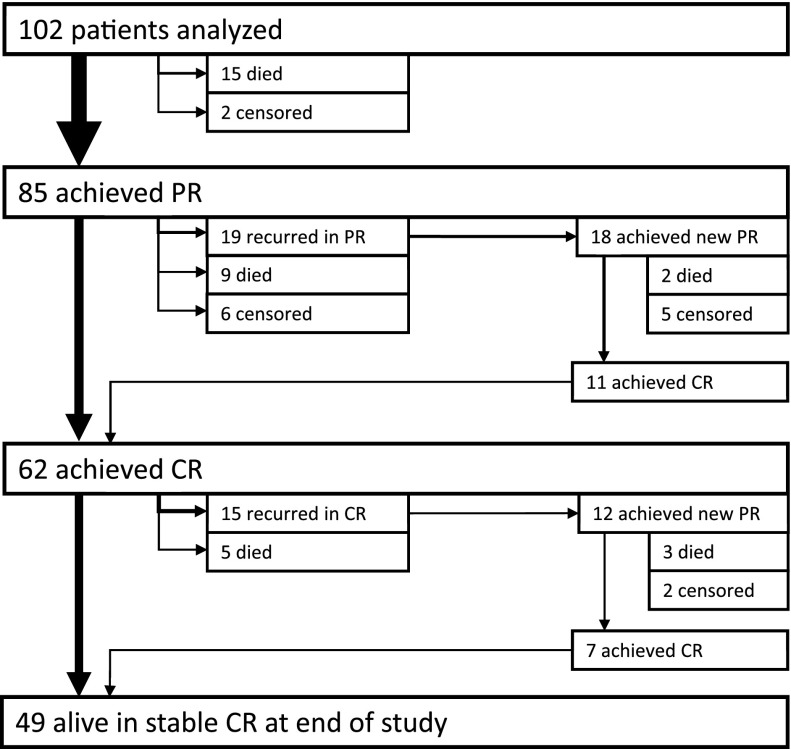
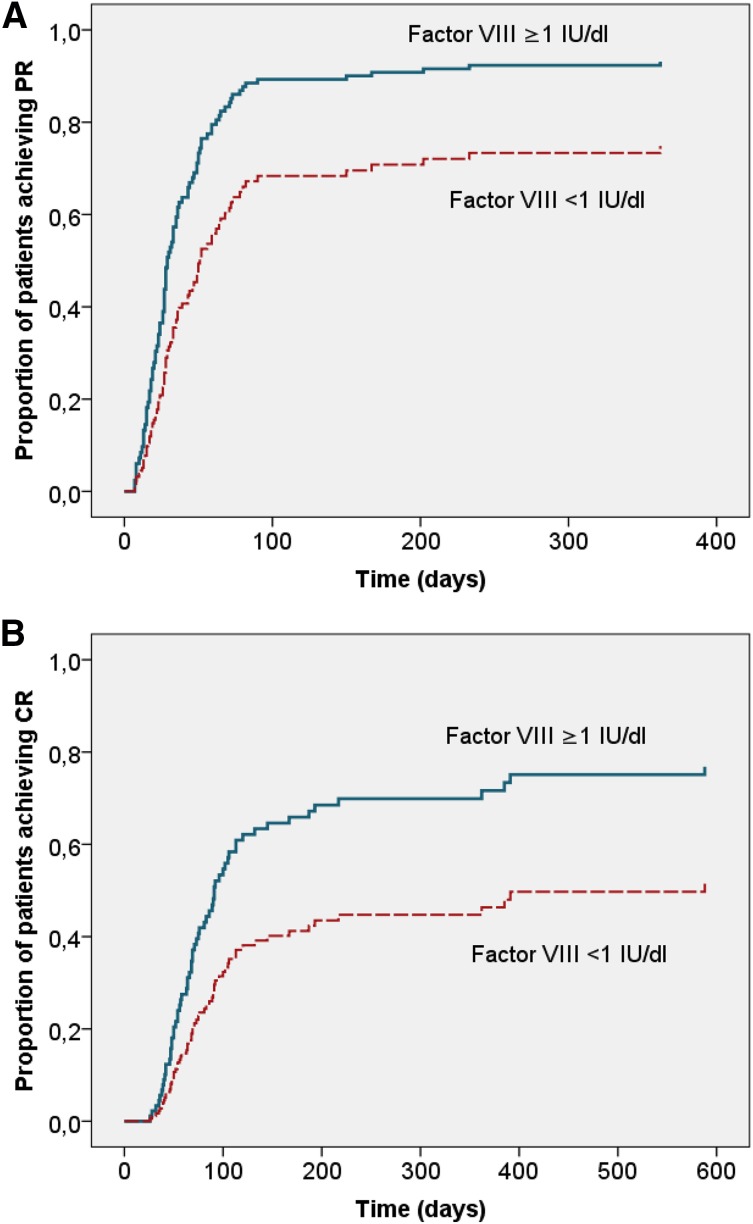
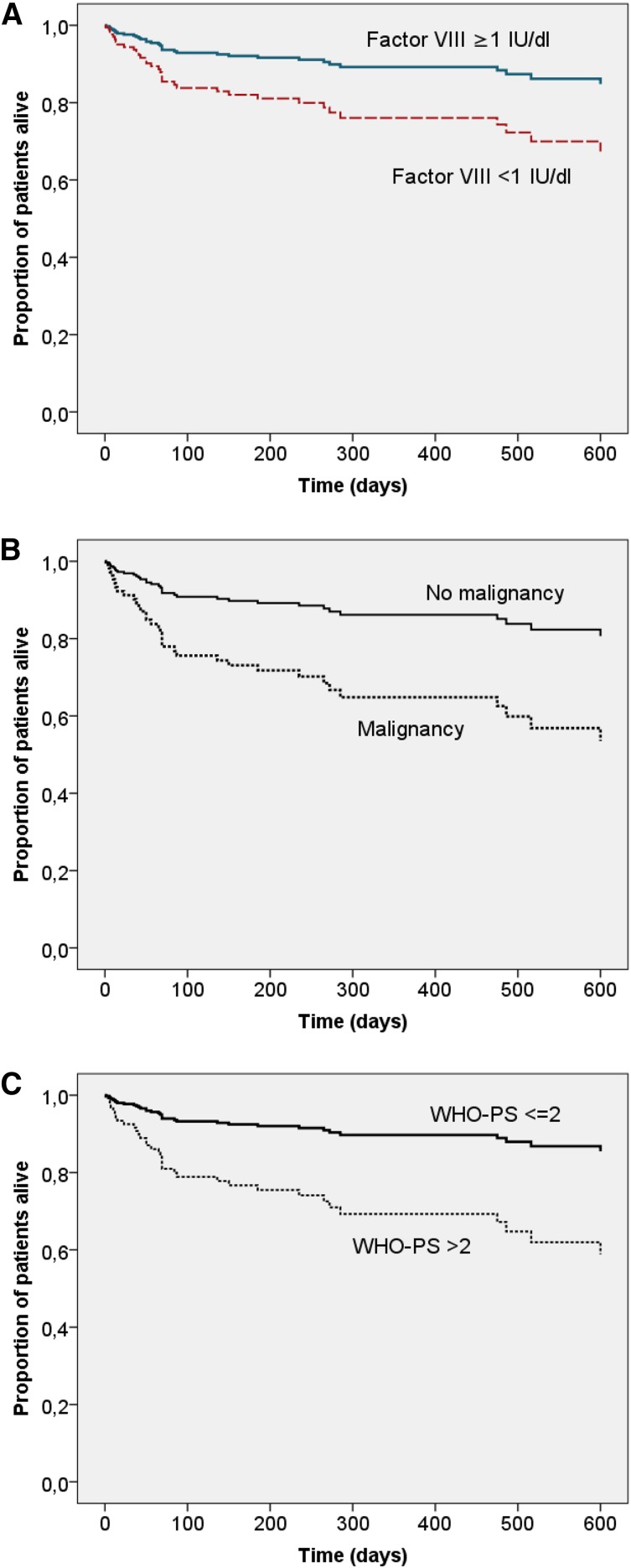
Acquired hemophilia A (AHA) is caused by autoantibodies against factor VIII (FVIII). Immunosuppressive treatment (IST) results in remission of disease in 60% to 80% of patients over a period of days to months. IST is associated with frequent adverse events, including infections as a leading cause of death. Predictors of time to remission could help guide IST intensity but have not been established. We analyzed prognostic factors in 102 prospectively enrolled patients treated with a uniform IST protocol. Partial remission (PR; defined as no active bleeding, FVIII restored >50 IU/dL, hemostatic treatment stopped >24 hours) was achieved by 83% of patients after a median of 31 days (range 7-362). Patients with baseline FVIII <1 IU/dL achieved PR less often and later (77%, 43 days) than patients with ≥1 IU/dL (89%, 24 days). After adjustment for other baseline characteristics, low FVIII remained associated with a lower rate of PR (hazard ratio 0.52, 95% confidence interval 0.33-0.81, P < .01). In contrast, PR achieved on steroids alone within ≤21 days was more common in patients with FVIII ≥1 IU/dL and inhibitor concentration <20 BU/mL (odds ratio 11.2, P < .0001). Low FVIII was also associated with a lower rate of complete remission and decreased survival. In conclusion, presenting FVIII and inhibitor concentration are potentially useful to tailor IST in AHA.
© 2015 by The American Society of Hematology.
Figures
Comment in
-
The problem of acquired hemophilia.Blood. 2015 Feb 12;125(7):1052-3. doi: 10.1182/blood-2014-12-618959. Blood. 2015. PMID: 25678432 No abstract available.
-
The anti-CD20 monoclonal antibody rituximab to treat acquired haemophilia A.Blood Transfus. 2016 May;14(2):255-61. doi: 10.2450/2015.0090-15. Epub 2015 Sep 3. Blood Transfus. 2016. PMID: 26509821 Free PMC article. Review.
References
-
- Collins PW. Therapeutic challenges in acquired factor VIII deficiency. Hematology Am Soc Hematol Educ Program. 2012;2012:369–374. - PubMed
-
- Franchini M, Mannucci PM. Acquired haemophilia A: a 2013 update. Thromb Haemost. 2013;110(6):1114–1120. - PubMed
-
- Knoebl P, Marco P, Baudo F, et al. EACH2 Registry Contributors. Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2). J Thromb Haemost. 2012;10(4):622–631. - PubMed
-
- Baudo F, Collins P, Huth-Kühne A, et al. EACH2 registry contributors. Management of bleeding in acquired hemophilia A: results from the European Acquired Haemophilia (EACH2) Registry. Blood. 2012;120(1):39–46. - PubMed
-
- Tengborn L, Baudo F, Huth-Kühne A, et al. EACH2 registry contributors. Pregnancy-associated acquired haemophilia A: results from the European Acquired Haemophilia (EACH2) registry. BJOG. 2012;119(12):1529–1537. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
