

Peripheral limb vascular malformations: an update of appropriate imaging and treatment options of a challenging condition
- PMID: 25525685
- PMCID: PMC4651202
- DOI: 10.1259/bjr.20140406
Peripheral limb vascular malformations: an update of appropriate imaging and treatment options of a challenging condition
Abstract
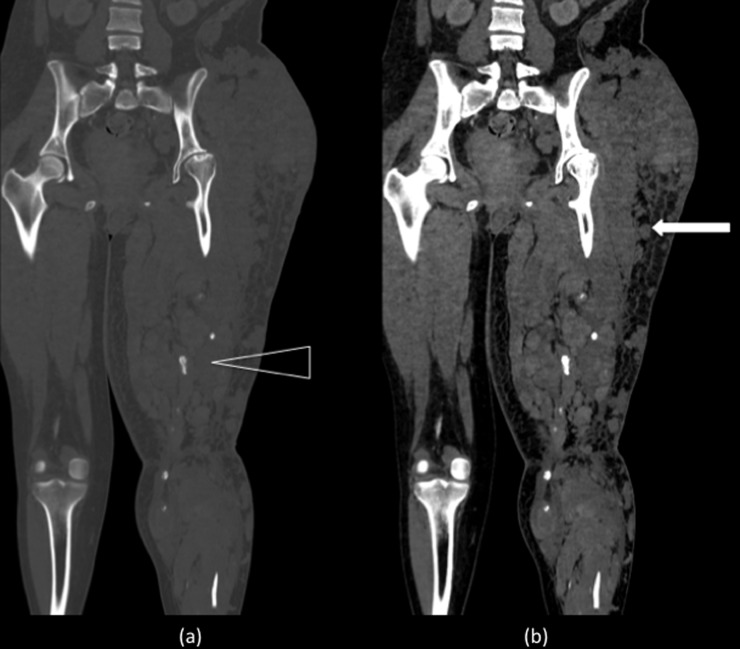
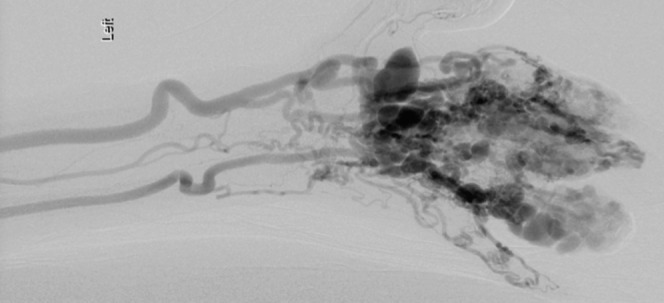
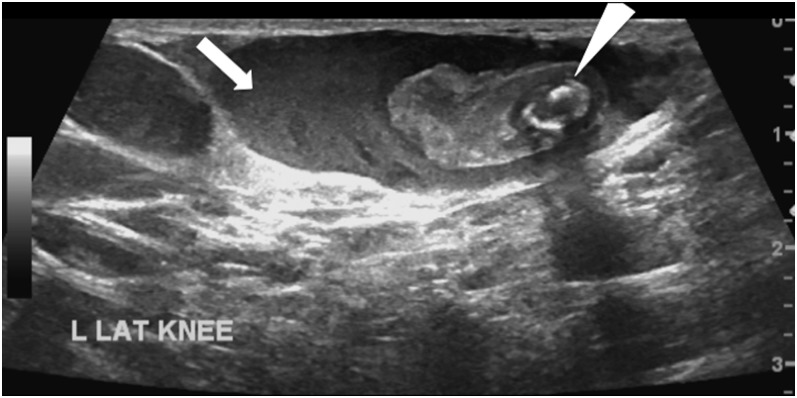
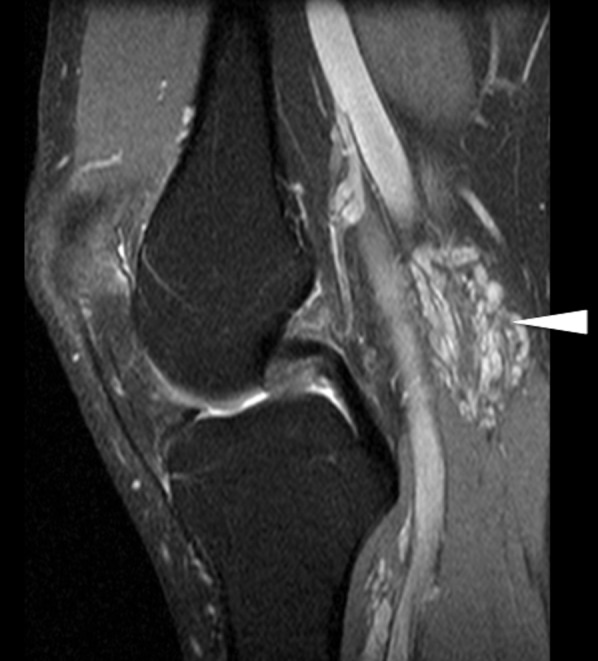
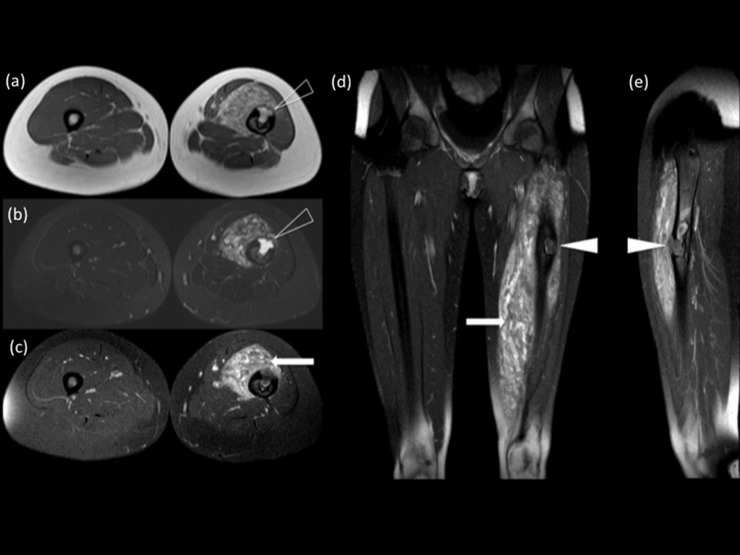
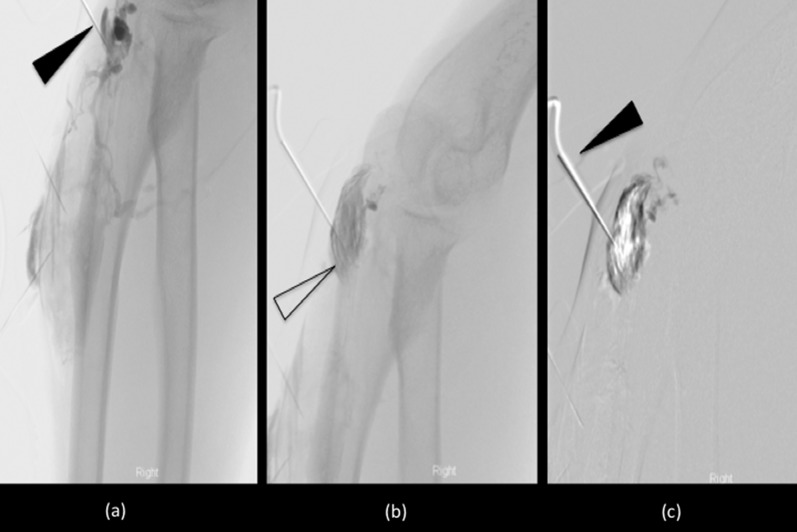
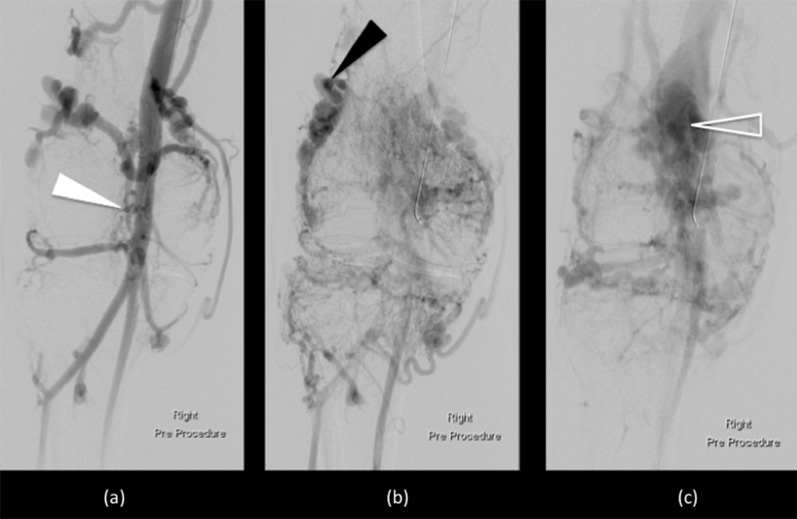
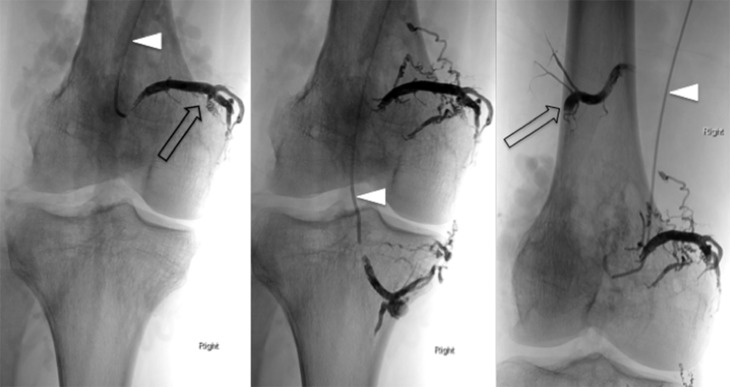
Peripheral vascular malformations encompass a wide spectrum of lesions that can present as an incidental finding or produce potentially life- or limb-threatening complications. They can have intra-articular and intraosseous extensions that will result in more diverse symptomology and present greater therapeutic challenges. Developments in classification, imaging and interventional techniques have helped to improve outcome. The onus is now placed on appropriate detailed preliminary imaging, diagnosis and classification to direct management and exclude other more common mimics. Radiologists are thus playing an increasingly important role in the multidisciplinary teams charged with the care of these patients. By fully understanding the imaging characteristics and image-guided procedures available, radiologists will be armed with the tools to meet these responsibilities. This review highlights the recent advances made in imaging and the options available in interventional therapy.
Figures

References
-
- Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 1982; 69: 412–22. - PubMed
-
- Mulliken JB, Glowacki J. Classification of pediatric vascular lesions. Plast Reconstr Surg 1982; 70: 120–1. - PubMed
-
- Legiehn GM, Heran MK. Classification, diagnosis, and interventional radiologic management of vascular malformations. Orthop Clin North Am 2006; 37: 435–74. - PubMed
-
- Hyodoh H, Hori M, Akiba H, Tamakawa M, Hyodoh K, Hareyama M. Peripheral vascular malformations imaging, treatment approaches, and therapeutic issues. Radiographics 2005; 25(Suppl 1): S159–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
