

The new IASLC-ATS-ERS lung adenocarcinoma classification: what the surgeon should know
- PMID: 25527015
- PMCID: PMC4272758
- DOI: 10.1053/j.semtcvs.2014.09.002
The new IASLC-ATS-ERS lung adenocarcinoma classification: what the surgeon should know
Abstract
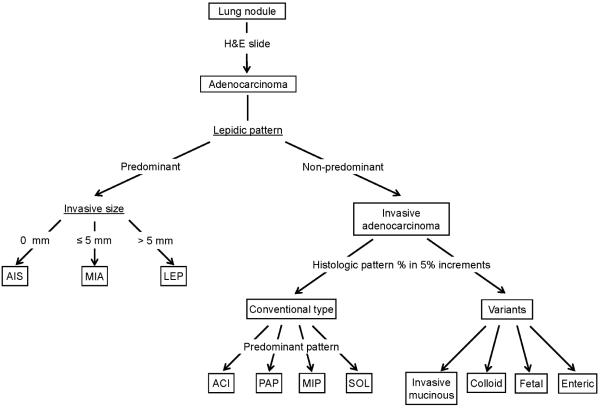
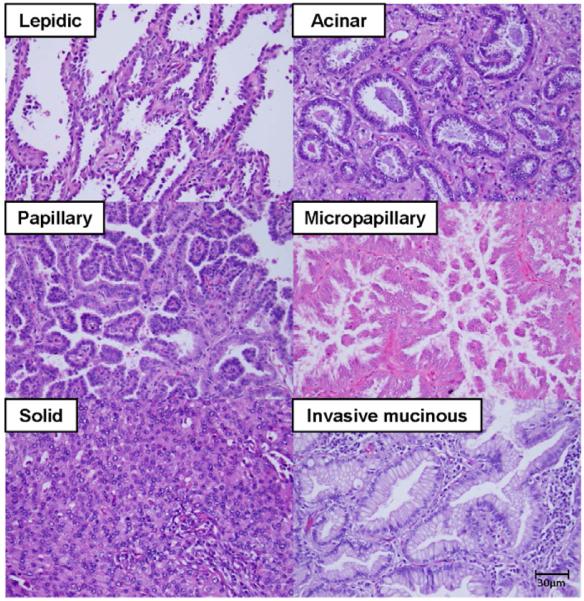
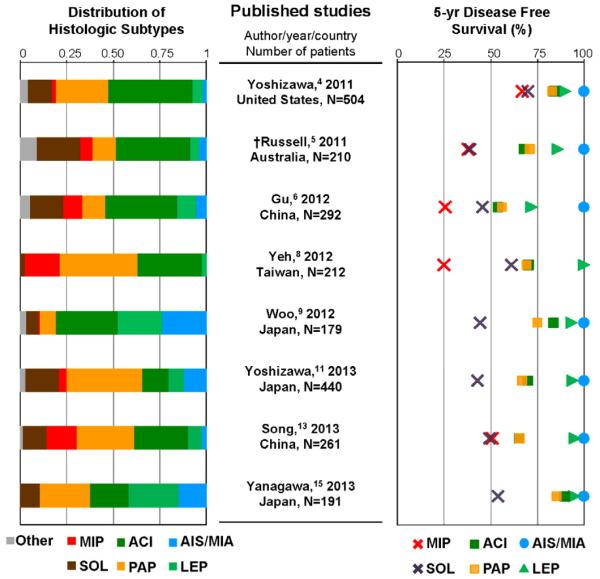
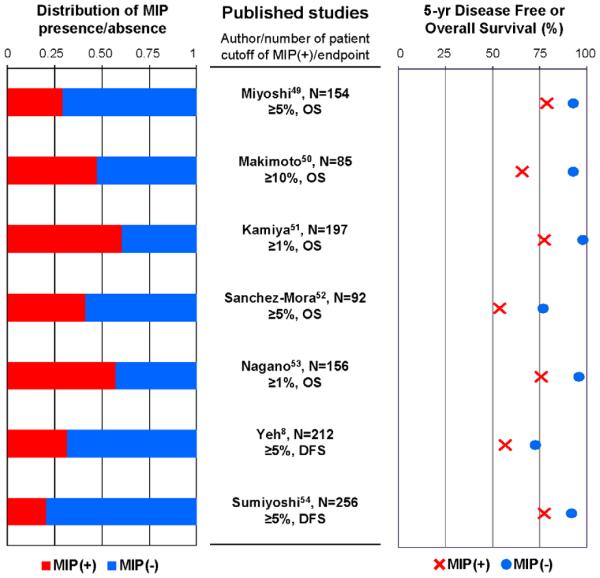
In 2011, a new histologic classification of lung adenocarcinomas was proposed from a joint working group of the International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society, based on the recommendation of an international and multidisciplinary panel. This classification proposed a method of comprehensive histologic subtyping (lepidic, acinar, papillary, micropapillary, and solid pattern) based on semiquantitative assessment of histologic patterns (in 5% increments), with the ultimate goal of choosing a single, predominant pattern. Prognostic subsets could then be described for the classification. Patients with completely resected adenocarcinoma in situ and minimally invasive adenocarcinomas experienced low risk of recurrence. Patients with micropapillary or solid predominant tumors have a high risk of recurrence or cancer-related death. Patients with acinar and papillary predominant tumors comprise an intermediate-risk group. Herein, we review the outline of the proposed International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society classification, a summary of published validation studies of this new classification, and then discuss the key surgical issues; we mainly focused on limited resection as an adequate treatment for early-stage lung adenocarcinomas, as well as preoperative and intraoperative diagnoses. We also review the published studies that identified the importance of histologic subtypes in predicting recurrence, both rates and patterns, in early-stage lung adenocarcinomas. This new classification for the most common type of lung cancer is useful for surgeons, as its implementation would require only hematoxylin-and-eosin histology slides, which is the common type of stain used in hospitals. It can be implemented with routine pathology evaluation and with no additional costs.
Keywords: histologic classification; limited resection; lung adenocarcinoma; micropapillary; small lung nodules.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6:244–85. - PMC - PubMed
-
- Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Annals of surgical oncology. 2010;17:1471–4. - PubMed
-
- Yoshizawa A, Motoi N, Riely GJ, Sima CS, Gerald WL, Kris MG, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011;24:653–64. - PubMed
-
- Russell PA, Wainer Z, Wright GM, Daniels M, Conron M, Williams RA. Does lung adenocarcinoma subtype predict patient survival?: A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J Thorac Oncol. 2011;6:1496–504. - PubMed
-
- Gu J, Lu C, Guo J, Chen L, Chu Y, Ji Y, et al. Prognostic significance of the IASLC/ATS/ERS classification in Chinese patients-A single institution retrospective study of 292 lung adenocarcinoma. J Surg Oncol. 2013;107:474–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
