

Vitamin D status is associated with mortality, morbidity, and growth failure among a prospective cohort of HIV-infected and HIV-exposed Tanzanian infants
- PMID: 25527666
- PMCID: PMC4264018
- DOI: 10.3945/jn.114.201566
Vitamin D status is associated with mortality, morbidity, and growth failure among a prospective cohort of HIV-infected and HIV-exposed Tanzanian infants
Abstract
Background: Vitamin D is a potent immunomodulator, but its impact on morbidity and mortality among infants remains unclear.
Objective: The objective of the study was to prospectively assess the association of vitamin D status with mortality, morbidity, and growth during the first 2 y of life.
Methods: A prospective cohort of 253 HIV-infected and 948 HIV-exposed Tanzanian infants enrolled in a randomized trial of multivitamins (not including vitamin D) was studied. Serum 25-hydroxyvitamin D [25(OH)D] concentrations were measured at 5-7 wk of age and infants were followed at monthly clinic visits until 24 mo. Physicians performed a clinical exam every 3 mo or when an illness was noted.
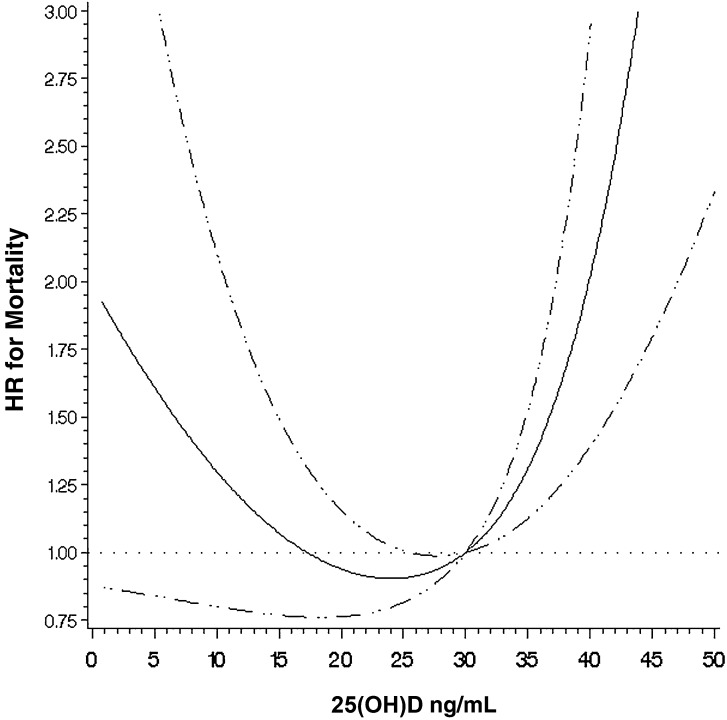
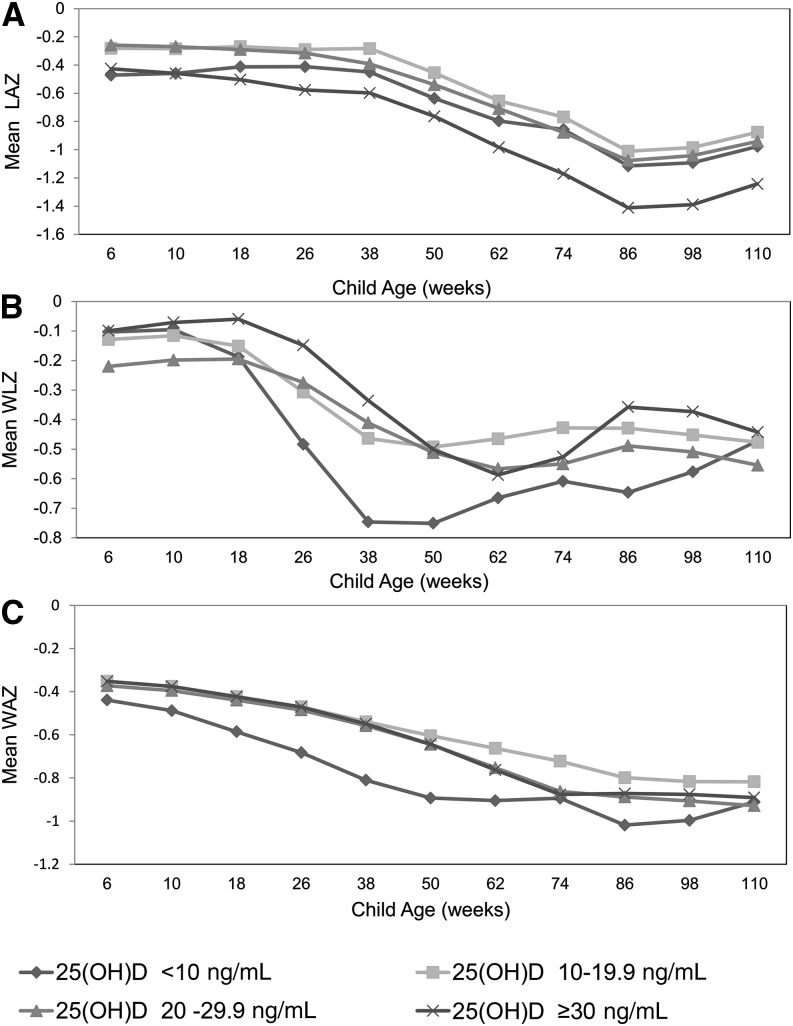
Results: Serum 25(OH)D concentrations were (means ± SDs) 18.6 ± 10.3 ng/mL and 18.1 ± 9.2 ng/mL for HIV-infected and HIV-exposed infants, respectively. Unexpectedly, serum 25(OH)D concentrations ≥30 ng/mL were significantly associated with higher mortality as compared to the 20-29.9 ng/mL reference for HIV-infected (HR: 2.47; 95% CI: 1.13, 5.44; P = 0.02) and HIV-exposed (HR: 4.00; 95% CI: 1.67, 9.58; P < 0.01) infants after multivariate adjustment. We found no statistically significant association between 25(OH)D concentrations <10 ng/mL and mortality for HIV-infected (HR: 1.43; 95% CI: 0.74, 2.78; P = 0.29) and HIV-exposed (HR: 1.56; 95% CI: 0.60, 4.03; P = 0.36) infants. Among HIV-exposed infants, 25(OH)D concentrations ≥30 ng/mL were significantly associated with clinical [incidence ratio rate (IRR): 1.34; 95% CI: 1.06,1.70; P = 0.02] and confirmed (IRR: 1.71; 95% CI: 1.71; 1.15, 2.54; P < 0.01) malaria diagnoses, whereas concentrations of <10 ng/mL were associated with oral candidiasis (IRR: 1.47; 95% CI: 1.00-2.15; P = 0.046) and wasting (HR: 1.71; 95% CI: 1.20, 2.43; P < 0.01).
Conclusion: The observational design of this study does not allow for causal interpretation; however, the results indicate a strong need for additional studies of vitamin D among HIV-infected and -exposed children, particularly in malaria-endemic settings. The parent trial was registered at clinicaltrials.gov as NCT00197730.
Keywords: HIV; child nutrition sciences; cohort studies; infant; malaria; micronutrients; vitamin D.
© 2015 American Society for Nutrition.
Conflict of interest statement
Author disclosures: CR Sudfeld, C Duggan, S Aboud, R Kupka, KP Manji, R Kisenge, and WW Fawzi, no conflicts of interest. R Kupka is a UNICEF staff member. The opinions and statements in this article are those of the authors and may not reflect official UNICEF policies.
Figures
References
-
- Filteau S. The HIV-exposed, uninfected African child. Trop Med Int Health 2009;14:276–87. - PubMed
-
- Villamor E. A potential role for vitamin D on HIV infection? Nutr Rev 2006;64:226–33. - PubMed
-
- Muhe L, Lulseged S, Mason KE, Simoes EA. Case-control study of the role of nutritional rickets in the risk of developing pneumonia in Ethiopian children. Lancet 1997;349:1801–4. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
