

An epidemiological evaluation of pediatric long bone fractures - a retrospective cohort study of 2716 patients from two Swiss tertiary pediatric hospitals
- PMID: 25528249
- PMCID: PMC4302599
- DOI: 10.1186/s12887-014-0314-3
An epidemiological evaluation of pediatric long bone fractures - a retrospective cohort study of 2716 patients from two Swiss tertiary pediatric hospitals
Abstract
Background: Children and adolescents are at high risk of sustaining fractures during growth. Therefore, epidemiological assessment is crucial for fracture prevention. The AO Comprehensive Injury Automatic Classifier (AO COIAC) was used to evaluate epidemiological data of pediatric long bone fractures in a large cohort.
Methods: Data from children and adolescents with long bone fractures sustained between 2009 and 2011, treated at either of two tertiary pediatric surgery hospitals in Switzerland, were retrospectively collected. Fractures were classified according to the AO Pediatric Comprehensive Classification of Long Bone Fractures (PCCF).
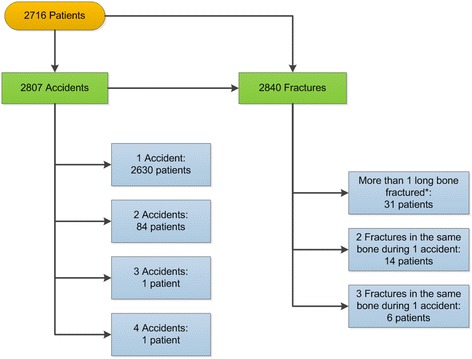
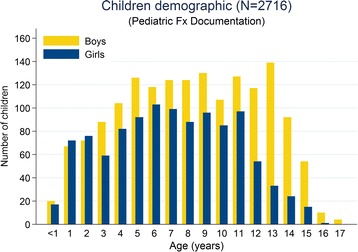
Results: For a total of 2716 patients (60% boys), 2807 accidents with 2840 long bone fractures (59% radius/ulna; 21% humerus; 15% tibia/fibula; 5% femur) were documented. Children's mean age (SD) was 8.2 (4.0) years (6% infants; 26% preschool children; 40% school children; 28% adolescents). Adolescent boys sustained more fractures than girls (p < 0.001). The leading cause of fractures was falls (27%), followed by accidents occurring during leisure activities (25%), at home (14%), on playgrounds (11%), and traffic (11%) and school accidents (8%). There was boy predominance for all accident types except for playground and at home accidents. The distribution of accident types differed according to age classes (p < 0.001). Twenty-six percent of patients were classed as overweight or obese - higher than data published by the WHO for the corresponding ages - with a higher proportion of overweight and obese boys than in the Swiss population (p < 0.0001).
Conclusion: Overall, differences in the fracture distribution were sex and age related. Overweight and obese patients seemed to be at increased risk of sustaining fractures. Our data give valuable input into future development of prevention strategies. The AO PCCF proved to be useful in epidemiological reporting and analysis of pediatric long bone fractures.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
