

Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of 168 Randomized Placebo-Controlled Trials
- PMID: 25528757
- PMCID: PMC4466178
- DOI: 10.1093/schbul/sbu170
Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of 168 Randomized Placebo-Controlled Trials
Erratum in
-
Corrigendum: Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of Randomized Placebo-Controlled Trials.Schizophr Bull. 2022 May 7;48(3):721. doi: 10.1093/schbul/sbz071. Schizophr Bull. 2022. PMID: 31504973 Free PMC article. No abstract available.
Abstract
Objectives: Existing treatments for schizophrenia can improve positive symptoms, but it is unclear if they have any impact on negative symptoms. This meta-analysis was conducted to assess the efficacy of available treatments for negative symptoms in schizophrenia.
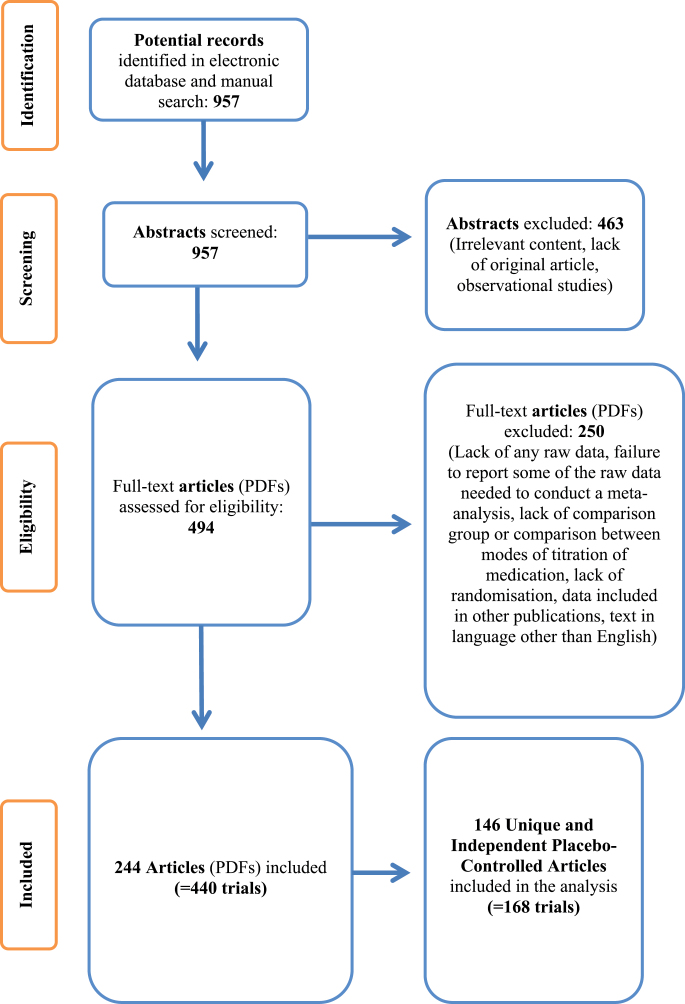
Methods: All randomized-controlled trials of interventions for negative symptoms in schizophrenia until December 2013 were retrieved; 168 unique and independent placebo-controlled trials were used. Negative symptom scores at baseline and follow-up, duration of illness, doses of medication, type of interventions, and sample demographics were extracted. Heterogeneity was addressed with the I (2) and Q statistic. Standardized mean difference in values of the Negative Symptom Rating Scale used in each study was calculated as the main outcome measure.
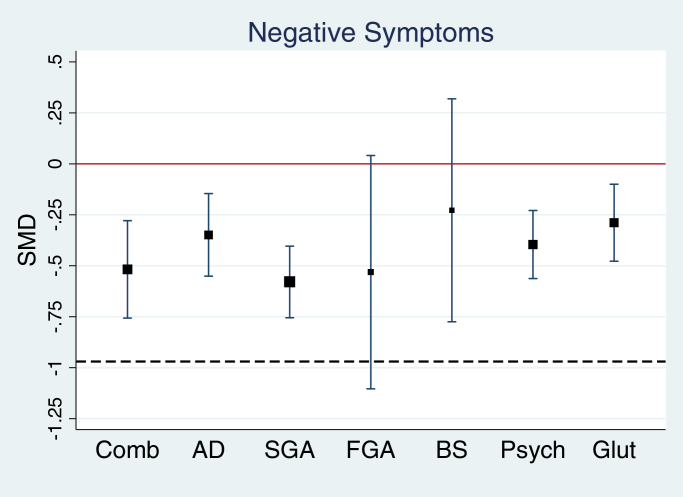
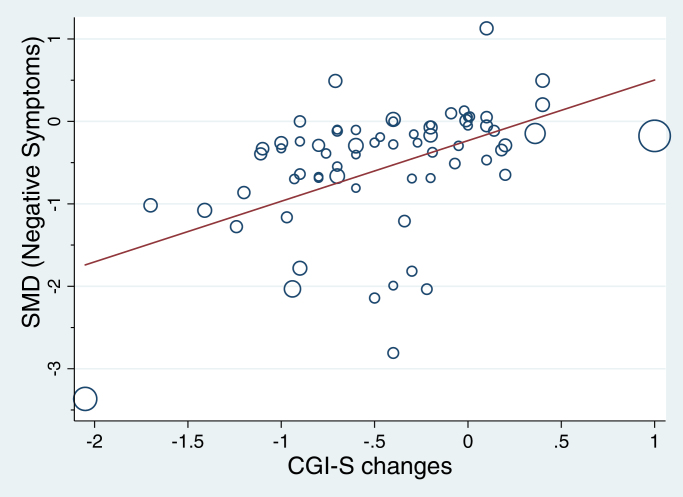
Results: 6503 patients in the treatment arm and 5815 patients in the placebo arm were included. No evidence of publication biases found. Most treatments reduced negative symptoms at follow-up relative to placebo: second-generation antipsychotics: -0.579 (-0.755 to -0.404); antidepressants: -0.349 (-0.551 to -0.146); combinations of pharmacological agents: -0.518 (-0.757 to -0.279); glutamatergic medications: -0.289 (-0.478 to -0.1); psychological interventions: -0.396 (-0.563 to -0.229). No significant effect was found for first-generation antipsychotics: -0.531 (-1.104 to 0.041) and brain stimulation: -0.228 (-0.775 to 0.319). Effects of most treatments were not clinically meaningful as measured on Clinical Global Impression Severity Scale.
Conclusions and relevance: Although some statistically significant effects on negative symptoms were evident, none reached the threshold for clinically significant improvement.
Keywords: antipsychotics; negative symptoms; psychosis; schizophrenia; treatment.
© The Author 2014. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Buchanan RW, Carpenter WT. Domains of psychopathology: an approach to the reduction of heterogeneity in schizophrenia. J Nerv Ment Dis. 1994;182:193–204. - PubMed
-
- Carpenter W, Buchanan R. Domains of psychopathology relevant to the study of etiology and treatment of schizophrenia. In: Schulz SC, Tamminga CA, eds. Schizophrenia: Scientific Progress. New York: Oxford University Press; 1989:13–22.
-
- Strauss JS, Carpenter WT, Bartko JJ. Part III. Speculations on the processes that underlie schizophrenic symptoms and signs. Schizophr Bull. 1974;1:61–69. - PubMed
-
- Kraepelin E. Lecture III, Dementia Praecox. Lectures on Clinical Psychiatry. New York: William Wood; 1917:21–29.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
