

Prevalence of iron deficiency on ICU discharge and its relation with fatigue: a multicenter prospective study
- PMID: 25529060
- PMCID: PMC4219000
- DOI: 10.1186/s13054-014-0542-9
Prevalence of iron deficiency on ICU discharge and its relation with fatigue: a multicenter prospective study
Abstract
Introduction: Prevalence of iron deficiency (ID) at intensive care (ICU) admission is around 25 to 40%. Blood losses are important during ICU stay, leading to iron losses, but prevalence of ID at ICU discharge is unknown. ID has been associated with fatigue and muscular weakness, and may thus impair post-ICU rehabilitation. This study assessed ID prevalence at ICU discharge, day 28 (D28) and six months (M6) after and its relation with fatigue.
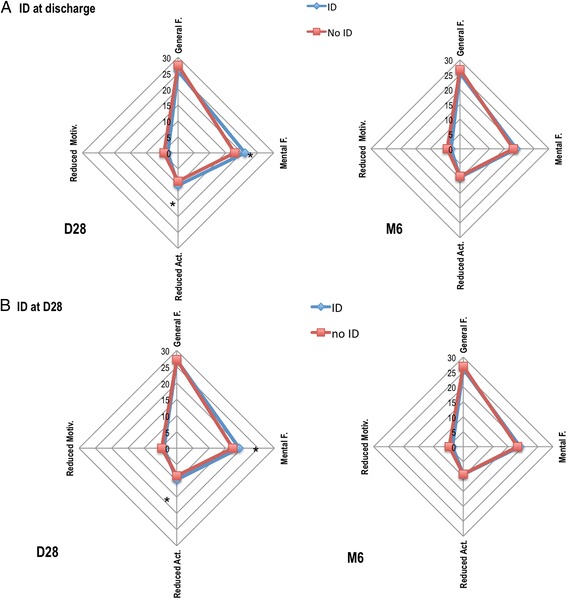
Methods: We conducted this prospective, multicenter observational study at four University hospitals ICUs. Anemic (hemoglobin (Hb) less than 13 g/dL in male and less than 12 g/dL in female) critically ill adult patients hospitalized for at least five days had an iron profile taken at discharge, D28 and M6. ID was defined as ferritin less than 100 ng/L or less than 300 ng/L together with a transferrin saturation less than 20%. Fatigue was assessed by numerical scale and the Multidimensional Fatigue Inventory-20 questionnaire at D28 and M6 and muscular weakness by a hand grip test at ICU discharge.
Results: Among 107 patients (men 77%, median (IQR) age 63 (48 to 73) years) who had a complete iron profile at ICU discharge, 9 (8.4%) had ID. At ICU discharge, their hemoglobin concentration (9.5 (87.7 to 10.3) versus 10.2 (92.2 to 11.7) g/dL, P =0.09), hand grip strength (52.5 (30 to 65) versus 49.5 (15.5 to 67.7)% of normal value, P =0.61) and visual analog scale fatigue scale (57 (40 to 80) versus 60 (47.5 to 80)/100, P =0.82) were not different from non-ID patients. At D28 (n =80 patients) and M6 (n =78 patients), ID prevalence increased (to 25 and 35% respectively) while anemia prevalence decreased (from 100% to 80 and 25% respectively, P <0.0001). ID was associated with increased fatigue at D28, after adjustment for main confounding factors, including anemia (regression coefficient (95%CI), 3.19 (0.74 to 5.64), P =0.012). At M6, this association disappeared.
Conclusions: The prevalence of ID increases from 8% at discharge to 35% six months after prolonged ICU stay (more than five days). ID was associated with increased fatigue, independently of anemia, at D28.
Figures


References
-
- Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Abraham E, MacIntyre NR, Shabot MM, Duh MS, Shapiro MJ. The CRIT Study: anemia and blood transfusion in the critically ill–current clinical practice in the United States. Crit Care Med. 2004;32:39–52. doi: 10.1097/01.CCM.0000104112.34142.79. - DOI - PubMed
-
- From the Centers for Disease Control and Prevention. Iron deficiency-United States, 1999-2000.JAMA 2002, 288:2114–2116. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
