

Mesenchymal stem (stromal) cells for treatment of ARDS: a phase 1 clinical trial
- PMID: 25529339
- PMCID: PMC4297579
- DOI: 10.1016/S2213-2600(14)70291-7
Mesenchymal stem (stromal) cells for treatment of ARDS: a phase 1 clinical trial
Abstract
Background: No effective pharmacotherapy for acute respiratory distress syndrome (ARDS) exists, and mortality remains high. Preclinical studies support the efficacy of mesenchymal stem (stromal) cells (MSCs) in the treatment of lung injury. We aimed to test the safety of a single dose of allogeneic bone marrow-derived MSCs in patients with moderate-to-severe ARDS.
Methods: The STem cells for ARDS Treatment (START) trial was a multicentre, open-label, dose-escalation, phase 1 clinical trial. Patients were enrolled in the intensive care units at University of California, San Francisco, CA, USA, Stanford University, Stanford, CA, USA, and Massachusetts General Hospital, Boston, MA, USA, between July 8, 2013, and Jan 13, 2014. Patients were included if they had moderate-to-severe ARDS as defined by the acute onset of the need for positive pressure ventilation by an endotracheal or tracheal tube, a PaO2:FiO2 less than 200 mm Hg with at least 8 cm H2O positive end-expiratory airway pressure (PEEP), and bilateral infiltrates consistent with pulmonary oedema on frontal chest radiograph. The first three patients were treated with low dose MSCs (1 million cells/kg predicted bodyweight [PBW]), the next three patients received intermediate dose MSCs (5 million cells/kg PBW), and the final three patients received high dose MSCs (10 million cells/kg PBW). Primary outcomes included the incidence of prespecified infusion-associated events and serious adverse events. The trial is registered with ClinicalTrials.gov, number NCT01775774.
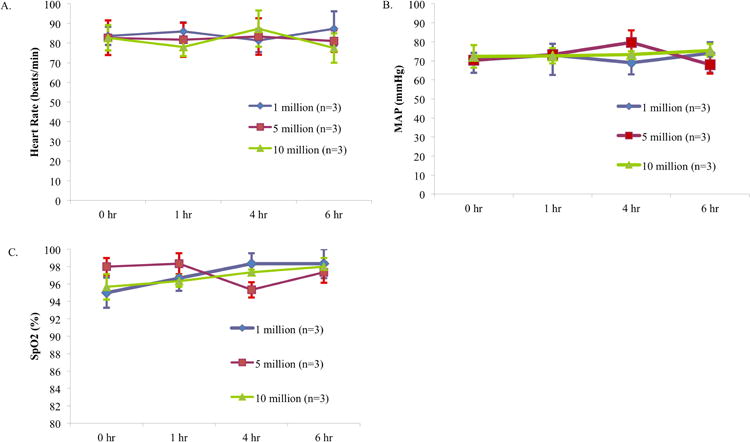
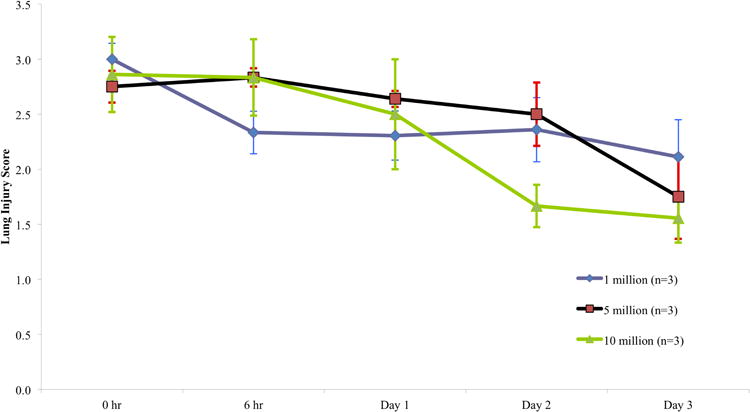
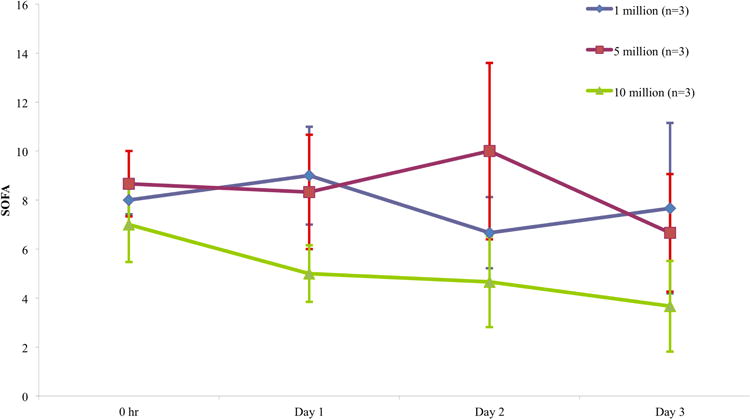
Findings: No prespecified infusion-associated events or treatment-related adverse events were reported in any of the nine patients. Serious adverse events were subsequently noted in three patients during the weeks after the infusion: one patient died on study day 9, one patient died on study day 31, and one patient was discovered to have multiple embolic infarcts of the spleen, kidneys, and brain that were age-indeterminate, but thought to have occurred before the MSC infusion based on MRI results. None of these severe adverse events were thought to be MSC-related.
Interpretation: A single intravenous infusion of allogeneic, bone marrow-derived human MSCs was well tolerated in nine patients with moderate to severe ARDS. Based on this phase 1 experience, we have proceeded to phase 2 testing of MSCs for moderate to severe ARDS with a primary focus on safety and secondary outcomes including respiratory, systemic, and biological endpoints.
Funding: The National Heart, Lung, and Blood Institute.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Cell therapies for ARDS: a promising start.Lancet Respir Med. 2015 Jan;3(1):2-3. doi: 10.1016/S2213-2600(14)70301-7. Epub 2014 Dec 17. Lancet Respir Med. 2015. PMID: 25529341 No abstract available.
-
Mesenchymal stem (stromal) cells for treatment of acute respiratory distress syndrome.Lancet Respir Med. 2015 Apr;3(4):e11-2. doi: 10.1016/S2213-2600(15)00049-1. Lancet Respir Med. 2015. PMID: 25890654 No abstract available.
-
Mesenchymal stem (stromal) cells for treatment of acute respiratory distress syndrome - authors' reply.Lancet Respir Med. 2015 Apr;3(4):e12-3. doi: 10.1016/S2213-2600(15)00040-5. Lancet Respir Med. 2015. PMID: 25890655 No abstract available.
-
Mesenchymal stem (stromal) cells for treatment of acute respiratory distress syndrome.Lancet Respir Med. 2015 Apr;3(4):e12. doi: 10.1016/S2213-2600(15)00047-8. Lancet Respir Med. 2015. PMID: 25890656 No abstract available.
References
-
- Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354:2564–2575. - PubMed
-
- Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–1116. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
