

Pathophysiology of spasticity: implications for neurorehabilitation
- PMID: 25530960
- PMCID: PMC4229996
- DOI: 10.1155/2014/354906
Pathophysiology of spasticity: implications for neurorehabilitation
Abstract
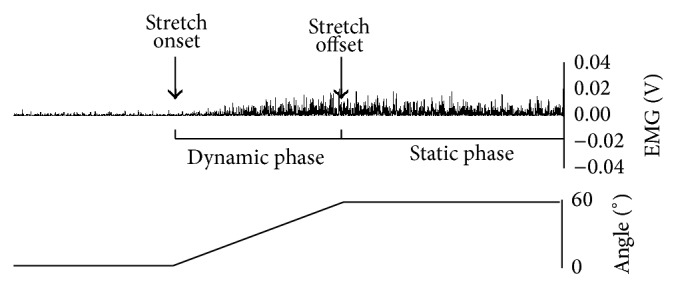
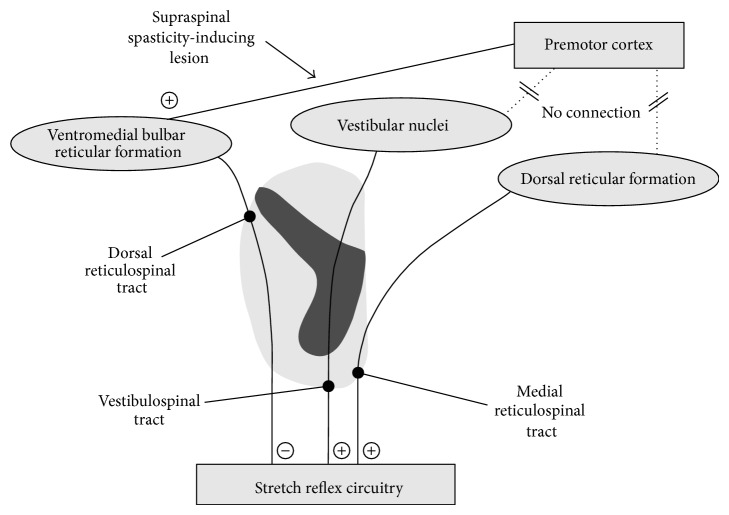
Spasticity is the velocity-dependent increase in muscle tone due to the exaggeration of stretch reflex. It is only one of the several components of the upper motor neuron syndrome (UMNS). The central lesion causing the UMNS disrupts the balance of supraspinal inhibitory and excitatory inputs directed to the spinal cord, leading to a state of disinhibition of the stretch reflex. However, the delay between the acute neurological insult (trauma or stroke) and the appearance of spasticity argues against it simply being a release phenomenon and suggests some sort of plastic changes, occurring in the spinal cord and also in the brain. An important plastic change in the spinal cord could be the progressive reduction of postactivation depression due to limb immobilization. As well as hyperexcitable stretch reflexes, secondary soft tissue changes in the paretic limbs enhance muscle resistance to passive displacements. Therefore, in patients with UMNS, hypertonia can be divided into two components: hypertonia mediated by the stretch reflex, which corresponds to spasticity, and hypertonia due to soft tissue changes, which is often referred as nonreflex hypertonia or intrinsic hypertonia. Compelling evidences state that limb mobilisation in patients with UMNS is essential to prevent and treat both spasticity and intrinsic hypertonia.
Figures
References
-
- Lance J. W. Symposium synopsis. In: Feldman R. G., Young R. R., Koella W. P., editors. Spasticity: Disordered Motor Control. 1980. pp. 485–494.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
