

Electromyographic permutation entropy quantifies diaphragmatic denervation and reinnervation
- PMID: 25532023
- PMCID: PMC4274091
- DOI: 10.1371/journal.pone.0115754
Electromyographic permutation entropy quantifies diaphragmatic denervation and reinnervation
Abstract
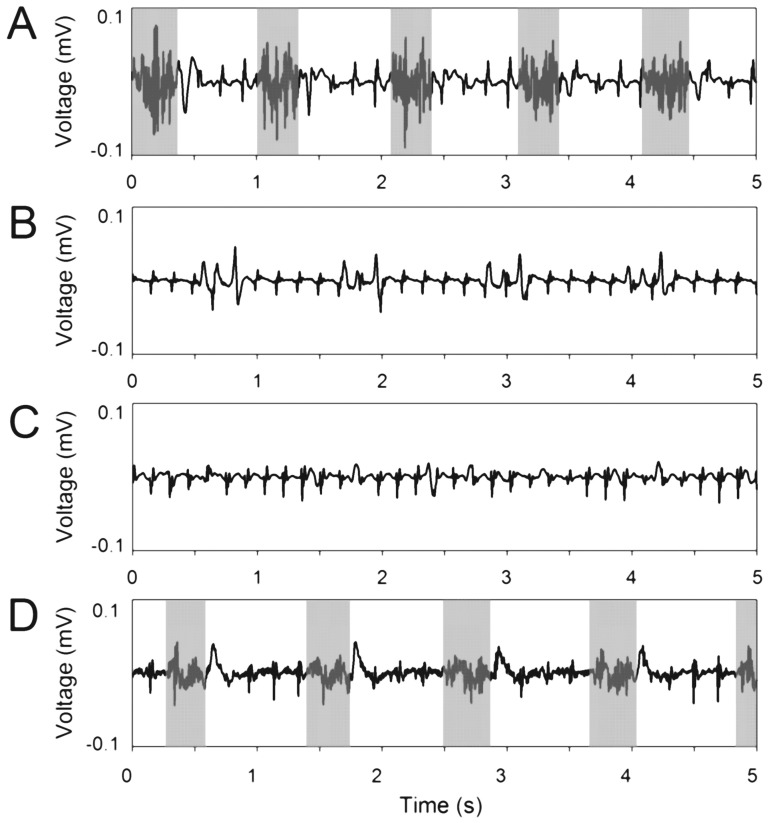
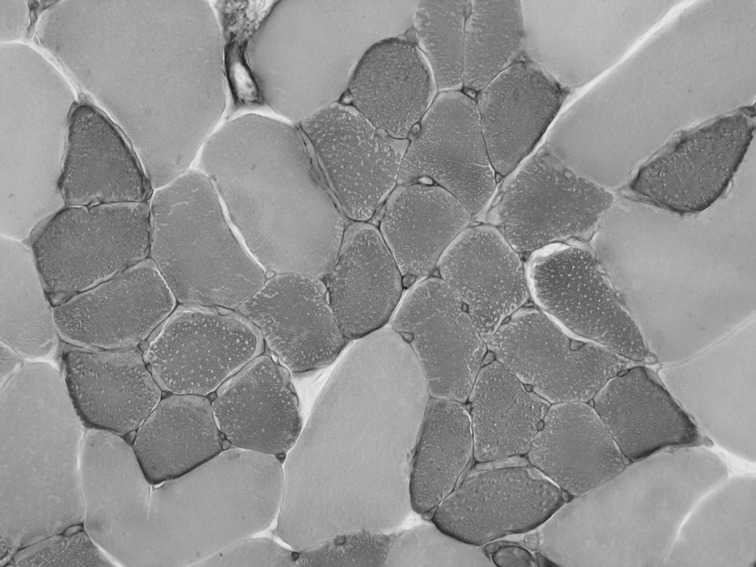
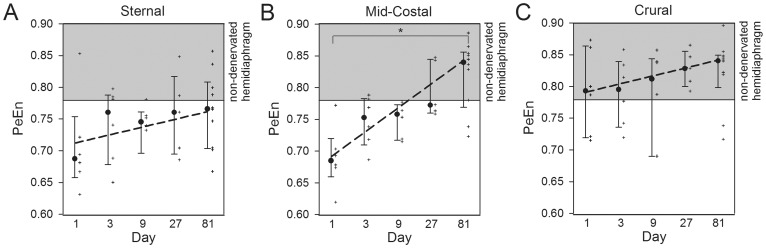
Spontaneous reinnervation after diaphragmatic paralysis due to trauma, surgery, tumors and spinal cord injuries is frequently observed. A possible explanation could be collateral reinnervation, since the diaphragm is commonly double-innervated by the (accessory) phrenic nerve. Permutation entropy (PeEn), a complexity measure for time series, may reflect a functional state of neuromuscular transmission by quantifying the complexity of interactions across neural and muscular networks. In an established rat model, electromyographic signals of the diaphragm after phrenicotomy were analyzed using PeEn quantifying denervation and reinnervation. Thirty-three anesthetized rats were unilaterally phrenicotomized. After 1, 3, 9, 27 and 81 days, diaphragmatic electromyographic PeEn was analyzed in vivo from sternal, mid-costal and crural areas of both hemidiaphragms. After euthanasia of the animals, both hemidiaphragms were dissected for fiber type evaluation. The electromyographic incidence of an accessory phrenic nerve was 76%. At day 1 after phrenicotomy, PeEn (normalized values) was significantly diminished in the sternal (median: 0.69; interquartile range: 0.66-0.75) and mid-costal area (0.68; 0.66-0.72) compared to the non-denervated side (0.84; 0.78-0.90) at threshold p<0.05. In the crural area, innervated by the accessory phrenic nerve, PeEn remained unchanged (0.79; 0.72-0.86). During reinnervation over 81 days, PeEn normalized in the mid-costal area (0.84; 0.77-0.86), whereas it remained reduced in the sternal area (0.77; 0.70-0.81). Fiber type grouping, a histological sign for reinnervation, was found in the mid-costal area in 20% after 27 days and in 80% after 81 days. Collateral reinnervation can restore diaphragm activity after phrenicotomy. Electromyographic PeEn represents a new, distinctive assessment characterizing intramuscular function following denervation and reinnervation.
Conflict of interest statement
Figures
Similar articles
-
Selective resection of the phrenic nerve roots in rabbits. Part I: Cartography of the residual innervation.Respir Physiol. 1997 Aug;109(2):127-38. doi: 10.1016/s0034-5687(97)00047-9. Respir Physiol. 1997. PMID: 9299644
-
Diaphragm recovery by laryngeal innervation after bilateral phrenicotomy or complete C2 spinal section in rats.Neurobiol Dis. 2006 Oct;24(1):53-66. doi: 10.1016/j.nbd.2006.05.002. Epub 2006 Jul 12. Neurobiol Dis. 2006. PMID: 16843001
-
Diaphragmatic effects of selective resection of the upper phrenic nerve root in dogs.Respir Physiol Neurobiol. 2006 Dec;154(3):419-30. doi: 10.1016/j.resp.2005.12.006. Epub 2006 Jun 9. Respir Physiol Neurobiol. 2006. PMID: 16762605
-
Respiratory muscle plasticity.Respir Physiol Neurobiol. 2005 Jul 28;147(2-3):235-51. doi: 10.1016/j.resp.2005.03.003. Respir Physiol Neurobiol. 2005. PMID: 15871925 Review.
-
Evaluation of phrenic nerve and diaphragm function with peripheral nerve stimulation and M-mode ultrasonography in potential pediatric phrenic nerve or diaphragm pacing candidates.Phys Med Rehabil Clin N Am. 2015 Feb;26(1):133-43. doi: 10.1016/j.pmr.2014.09.010. Phys Med Rehabil Clin N Am. 2015. PMID: 25479785 Review.
Cited by
-
Perfusion pressure as a determinant of respiratory function outcomes in unilateral biportal lumbar endoscopic procedures.Front Pharmacol. 2025 May 30;16:1593118. doi: 10.3389/fphar.2025.1593118. eCollection 2025. Front Pharmacol. 2025. PMID: 40520198 Free PMC article.
-
Clinical Anatomy and Diagnostic Challenges in Peripheral Nerve Trauma for the Forensic Physician.Diagnostics (Basel). 2025 Jun 24;15(13):1597. doi: 10.3390/diagnostics15131597. Diagnostics (Basel). 2025. PMID: 40647595 Free PMC article. Review.
References
-
- Elefteriades J, Singh M, Tang P, Siegel MD, Kenney B, et al. (2008) Unilateral diaphragm paralysis: etiology, impact, and natural history. J Cardiovasc Surg (Torino) 49:289–295. - PubMed
-
- Kaufman MR, Elkwood AI, Rose MI, Patel T, Ashinoff R, et al. (2011) Reinnervation of the paralyzed diaphragm: application of nerve surgery techniques following unilateral phrenic nerve injury. Chest 140:191–197. - PubMed
-
- Merino-Ramirez MA, Juan G, Ramon M, Cortijo J, Morcillo EJ (2007) Diaphragmatic paralysis following minor cervical trauma. Muscle Nerve 36:267–270. - PubMed
-
- Douglass BE, Clagett OT (1960) The prognosis in idiopathic diaphragmatic paralysis. Dis Chest 37:294–297. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
