

Prophylactic manual rotation for fetal malposition to reduce operative delivery
- PMID: 25532081
- PMCID: PMC11032750
- DOI: 10.1002/14651858.CD009298.pub2
Prophylactic manual rotation for fetal malposition to reduce operative delivery
Update in
-
Prophylactic manual rotation of the fetal head (manual rotation alone) to reduce operative delivery and complications for mother and babies.Cochrane Database Syst Rev. 2025 Jul 18;7(7):CD009298. doi: 10.1002/14651858.CD009298.pub3. Cochrane Database Syst Rev. 2025. PMID: 40678975
Abstract
Background: Manual rotation is commonly performed to increase the chances of normal vaginal delivery and is perceived to be safe. Manual rotation has the potential to prevent operative delivery and caesarean section, and reduce obstetric and neonatal complications.
Objectives: To assess the effect of prophylactic manual rotation for women with malposition in labour on mode of delivery, and maternal and neonatal outcomes.
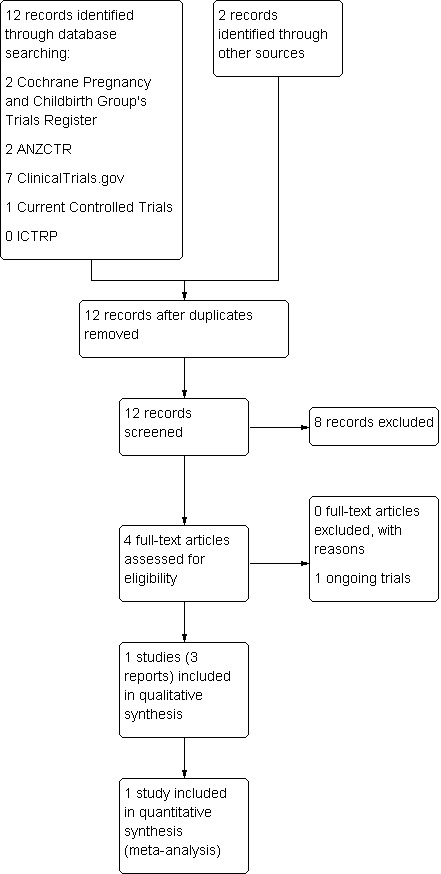
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 October 2014), the Australian and New Zealand Clinical Trials Registry (ANZCTR), ClinicalTrials.gov, Current Controlled Trials and the WHO International Clinical Trials Registry Platform (ICTRP) (all searched 23 February 2014), previous reviews and, references of retrieved studies.
Selection criteria: Randomised, quasi-randomised or cluster-randomised clinical trials comparing prophylactic manual rotation in labour for fetal malposition versus expectant management, augmentation of labour or operative delivery. We defined prophylactic manual rotation as rotation performed without immediate assisted delivery.
Data collection and analysis: Two review authors independently assessed study eligibility and quality, and extracted data.
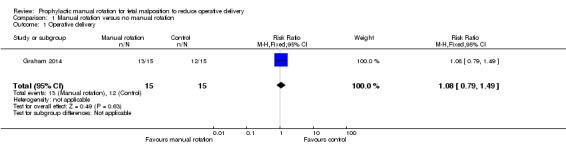
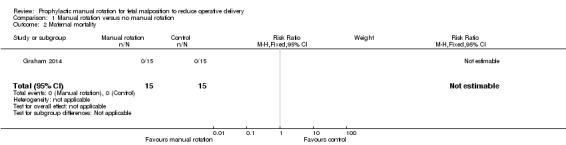
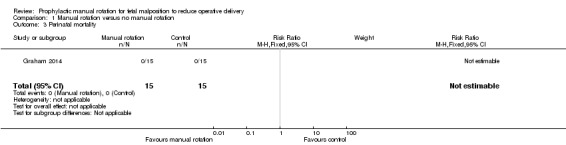
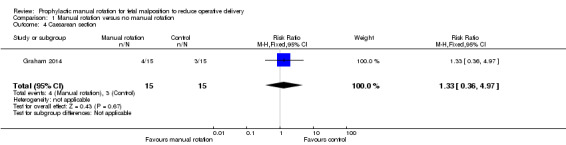
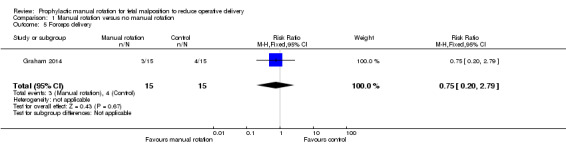
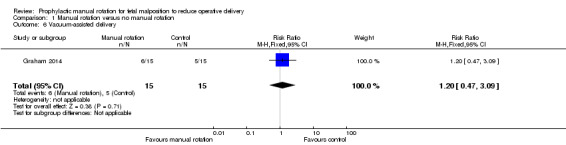
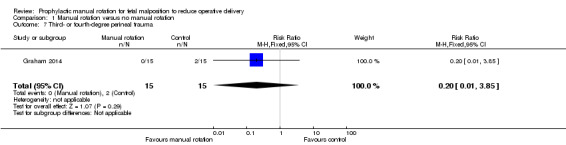
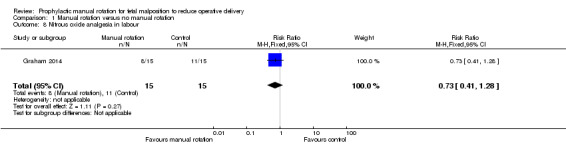
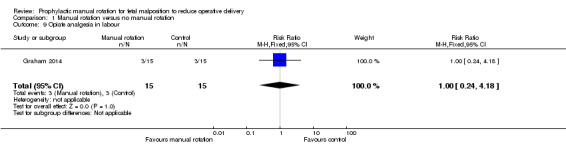
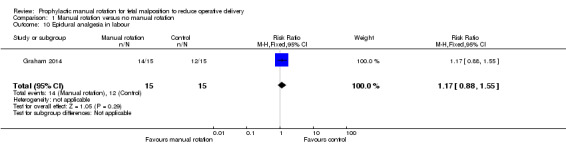
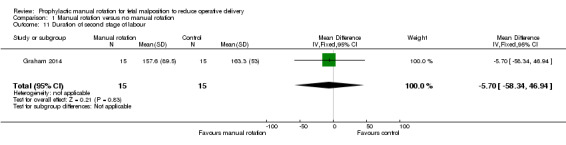
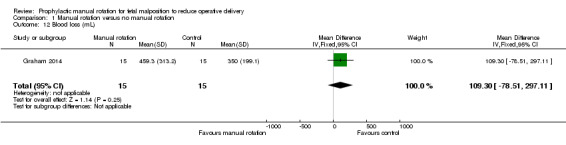
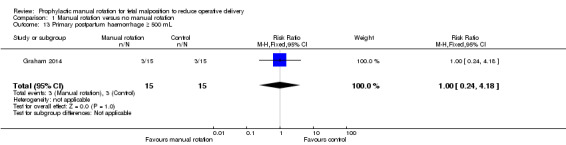
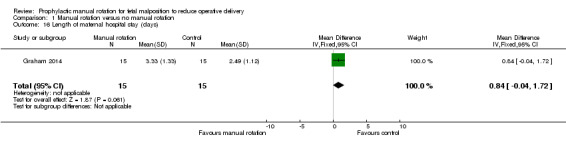
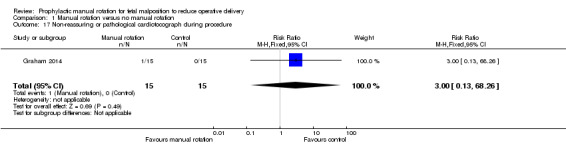
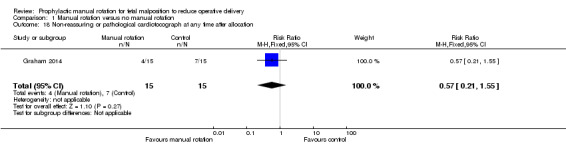
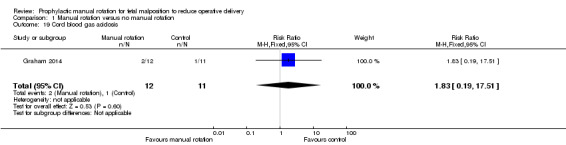
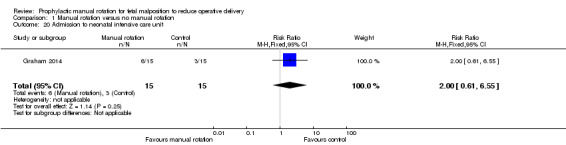
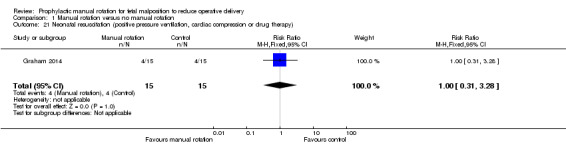
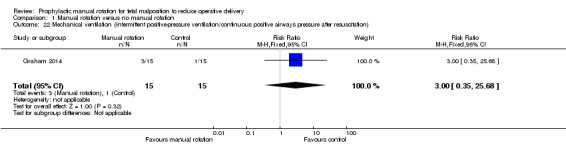
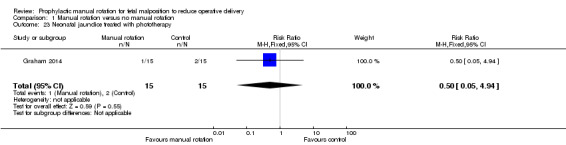
Main results: We included only one small pilot study (involving 30 women). The study, which we considered to be at low risk of bias, was conducted in a tertiary referral hospital in Australia, and involved women with cephalic, singleton pregnancies. The primary outcome was operative delivery (instrumental delivery or caesarean section).In the manual rotation group, 13/15 women went on to have an instrumental delivery or caesarean section, whereas in the control group, 12/15 women had an operative delivery. The estimated risk ratio was 1.08 (95% confidence interval 0.79 to 1.49). There were no maternal or fetal mortalities in either groupThere were no clear differences for any of the secondary maternal or neonatal outcomes reported (e.g. perineal trauma, analgesia use duration of labour).In terms of adverse events, there were no reported cases of umbilical cord prolapse or cervical laceration and a single case of a non-reassuring or pathological cardiotocograph during the procedure.
Authors' conclusions: Currently, there is insufficient evidence to determine the efficacy of prophylactic manual rotation early in the second stage of labour for prevention of operative delivery. One additional study is ongoing. Further appropriately designed trials are required to determine the efficacy of manual rotation.
Conflict of interest statement
David A Osborn: none known.
Dr Bradley de Vries, Hala Phipps and Clinical Professor Jon Hyett were involved in the designing and conducting of the one study (pilot randomised controlled trial) included in this review (Graham 2014). Brad de Vries, Hala Phipps and Jon Hyett have an NHMRC (National Health and Medical Research Council) grant and are currently performing a randomised controlled trial to assess the efficacy of manual rotation for malposition in the second stage of labour for reducing operative delivery. This randomised controlled trial is potentially eligible for inclusion in this review. All decisions relating to the inclusion of this trial, as well as assessment of risk of bias and data extraction, will include a member of the review team (David Osborn) who is not directly involved in the trials.
Figures
References
References to studies included in this review
Graham 2014 {published data only}
-
- Graham K, Phipps H, Hyett JA, Ludlow JP, Mackie A, Marren A, et al. Persistent Occiput‐Posterior: OUTcomes following digital rotation: a pilot randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2014;54(3):268‐74. - PubMed
-
- Graham K, Phipps H, Hyett JA, Ludlow JP, Mackie A, Marren A, et al. Persistent occipito‐posterior position: outcomes following digital rotation. A pilot study. Ultrasound in Obstetrics & Gynecology 2012;40(Suppl 1):241.
-
- Phipps H. Persistent occipito‐posterior: outcomes following digital rotation. The "POPOUT" Study, 2011. Australian New Zealand Clinical Trials Registry (http://www.anzctr.org.au/trial_view.aspx?ACTRN=12609000833268) (accessed 31 August 2011) 2011.
References to ongoing studies
Phipps 2013 {published data only}
-
- Phipps H. Persistent Occiput Transverse: OUTcomes following manual rotation. Australian New Zealand Clinical Trials Registry (accessed 10 July 2013) 2013.
Additional references
ACOG 2001
-
- American College of Obstetrics and Gynecology. Operative vaginal delivery. Clinical management guidelines for obstetrician‐gynecologists. International Journal of Gynecology and Obstetrics 2001;74(1):69‐76. - PubMed
Akmal 2004
-
- Akmal S, Kametas N, Tsoi E, Howard R, Nicolaides KH. Ultrasonographic occiput position in early labour in the prediction of caesarean section. BJOG: an international journal of obstetrics and gynaecology 2004;111:532‐6. - PubMed
Benavides 2005
-
- Benavides L, Wu JM, Hundley AF, Invester TS, Viscose AG. The impact of occiput posterior fetal head position on the risk of anal sphincter injury in forceps‐assisted vaginal deliveries. American Journal of Obstetrics and Gynecology 2005;192:1702‐6. - PubMed
Cargill 2004
-
- Cargill YM, MacKinnon CJ, Arsenault M‐Y, Bartellas E, Daniels S, Gleason T. Guidelines for operative vaginal birth. Journal of Obstetrics & Gynaecology Canada 2004;26(4):747‐61. - PubMed
Cheng 2006a
-
- Cheng Y, Shaffer B, Caughey A. The association between persistent occiput posterior position and neonatal outcomes. Obstetrics & Gynecology 2006;107(4):837‐44. - PubMed
Cheng 2006b
-
- Cheng YW, Shaffer BL, Caughey AB. Associated factors and outcomes of persistent occiput posterior position: a retrospective cohort study from 1976 to 2001. Journal of Maternal‐Fetal and Neonatal Medicine 2006;19:563‐8. - PubMed
Cooper 2002
-
- Cooper GM, Lewis G, Neilson J. Confidential enquiries into maternal deaths, 1997‐1999. British Journal of Anaesthesia 2002;89(3):369‐72. - PubMed
Cunningham 1997
-
- Cunningham FG, MacDonald PC, Gant NF, Levenno KJ, Gistrap III LC, Hankins GD, et al. Williams Obstetrics. 20th Edition. Stamford, Connecticut: Appleton and Lange, 1997:448‐50.
Dasche 2002
-
- Dashe JS, McIntire DD, Ramus RM, Santos‐Ramos R, Twickler DM. Persistence of placenta previa according to gestational age at ultrasound. Obstetrics & Gynecology 2002;99:692‐7. - PubMed
De la Torre 2006
-
- Torre L, Conzales‐Quintero VH, Mayor‐Lynn K, Smarkusky L, Hoffman MC, Saab A, et al. Significance of accidental extensions in the lower uterine segment during caesarean delivery. American Journal of Obstetrics and Gynecology 2006;194:e4‐e6. - PubMed
Deneux‐Tharaux 2006
-
- Deneux‐Tharaux C, Carmona E, Bouvier‐Colle MH, Bréart G. Postpartum maternal mortality and caesarean delivery. Obstetrics & Gynecology 2006;108(3 Pt 1):541‐8. - PubMed
Fitzpatrick 2001
-
- Fitzpatrick M, McQuillan K, O'Herlihy C. Influence of persistent occiput posterior position on delivery outcome. Obstetrics & Gynecology 2001;98:1027‐31. - PubMed
Gilliam 2002
-
- Gilliam M, Rosenberg D, Davis F. The likelihood of placenta previa with greater number of cesarean deliveries and higher parity. Obstetrics & Gynecology 2002;99:976‐80. - PubMed
Hall 1999
-
- Hall M, Bewley S. Maternal mortality and mode of delivery. Lancet 1999;354:776. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hunter 2007
Laws 2010
-
- Laws PJ, Li Z, Sullivan EA. Australia's Mothers and Babies 2008. Perinatal Statistics Series no. 24. Cat. no. PER 50. Canberra: Australian Institute of Health and Welfare, 2010.
Le Ray 2007
-
- Ray C, Serres P, Schmitz T, Cabrol D, Goffinet F. Manual rotation in occiput posterior or transverse positions. Obstetrics & Gynecology 2007;110(4):873‐9. - PubMed
Lieberman 2005
-
- Lieberman E, Davidson K, Lee‐Parritz A, Shearer E. Changes in fetal position during labor and their association with epidural analgesia. Obstetrics & Gynecology 2005;105:974‐82. - PubMed
Lumbiganon 2010
-
- Lumbiganon P, Laopaiboon M, Gulmezoglu AM, Souza JP, Taneepanichskul S, Ruyan P, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007‐08. Lancet 2010;375:490‐9. - PubMed
Lyndon‐Rochelle 2001
-
- Lyndon‐Rochelle M, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior cesarean delivery. New England Journal of Medicine 2001;345:3‐8. - PubMed
Minkoff 2003
-
- Minkoff H, Chervenak FA. Elective primary cesarean delivery. New England Journal of Medicine 2003;348:946‐50. - PubMed
O'Driscoll 1984
-
- O'Driscoll K, M Foley, MacDonald D. Active management of labor as an alternative to cesarean section for dystocia. Obstetrics & Gynecology 1984;63(4):485‐90. - PubMed
Pearl 1993
-
- Pearl ML, Roberts JM, Laros RK, Hurd WW. Vaginal delivery from the persistent occiput posterior position. Influence on maternal and neonatal morbidity. Journal of Reproductive Medicine 1993;38:955‐61. - PubMed
Phipps 2011
Phipps 2012
-
- Phipps H, Vries B, Lee PN, Hyett J. A Survey of obstetric practices in the management of occipito‐posterior position in labour and delivery among obstetricians in Australia and New Zealand. Australian and New Zealand Journal of Obstetrics and Gynaecology 2012;52:450‐54. - PubMed
Phipps 2014
-
- Phipps H, Vries B, Jagadish U, Hyett J. Management of occiput posterior position in the second stage of labour: a survey of midwifery practice in Australia. Birth 2014;41(1):64‐69. - PubMed
Ponkey 2003
-
- Ponkey SE, Cohen AP, Heffner LJ, Lieberman E. Persistent fetal occiput posterior position: obstetric outcomes. Obstetrics & Gynecology 2003;101:915‐20. - PubMed
RevMan 2012 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Schuitemaker 1997
-
- Schuitemaker N, Van Roosmalenj, Dekker G, Dongen P, Geijn H, Gravenhorst JB. Maternal mortality after cesarean section in the Netherlands. Acta Obstetricia et Gynecologica Scandinavica 1997;76:332‐4. - PubMed
Senecal 2005
-
- Senecal J, Xiong X, Fraser WD. Effect of fetal position on second‐stage duration and labor outcome. Obstetrics & Gynecology 2005;105:763‐72. - PubMed
Shaffer 2011
-
- Shaffer BL, Cheng YW, Vargas JE, Caughey AB. Manual rotation to reduce caesarean delivery in occiput posterior or transverse position. Journal of Maternal‐Fetal and Neonatal Medicine 2011;24(1):65‐72. - PubMed
Sherer 2002
-
- Sherer D, Miodovnik M, Bradley K, Langer O. Intrapartum fetal head position 1: comparison between transvaginal digital examination and transabdominal ultrasound assessment during the active stage of labor. Ultrasound in Obstetrics and Gynecology 2002;19:258‐63. - PubMed
Simkin 2010
-
- Simkin, P. The fetal occiput posterior position: state of the science and a new perspective. Birth 2010;37(1):61‐71. - PubMed
Souka 2003
-
- Souka AP, Haritos T, Basayiannis K, Noikokyri N, Antsaklis A. Intrapartum ultrasound for the examination of the fetal head position in normal and obstructed labor. Journal of Maternal‐Fetal and Neonatal Medicine 2003;13:59‐63. - PubMed
Tarnier 1982
-
- Tarnier S, Chantreuil G. In: Lauwereyus H editor(s). Traitê de L'art des Accouchements (Tome 2). 2nd Edition. Paris: Figure, 1982.
To 2000
-
- To WWK, Li ICF. Occipital posterior and occipital transverse positions: reappraisal of the obstetric risks. Australian and New Zealand Journal of Obstetrics and Gynaecology 2000;40(3):275‐9. - PubMed
Wu 2005
-
- Wu JM, Williams KS, Hundley AF, Connolly A, Visco AG. Occiput posterior fetal head position increases the risk of anal sphincter injury in vacuum‐assisted deliveries. American Journal of Obstetrics and Gynecology 2005;193:525‐8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical