

Sympathetic nerve stimulation, not circulating norepinephrine, modulates T-peak to T-end interval by increasing global dispersion of repolarization
- PMID: 25532528
- PMCID: PMC4405126
- DOI: 10.1161/CIRCEP.114.002195
Sympathetic nerve stimulation, not circulating norepinephrine, modulates T-peak to T-end interval by increasing global dispersion of repolarization
Abstract
Background: T-peak to T-end interval (Tp-e) is an independent marker of sudden cardiac death. Modulation of Tp-e by sympathetic nerve activation and circulating norepinephrine is not well understood. The purpose of this study was to characterize endocardial and epicardial dispersion of repolarization (DOR) and its effects on Tp-e with sympathetic activation.
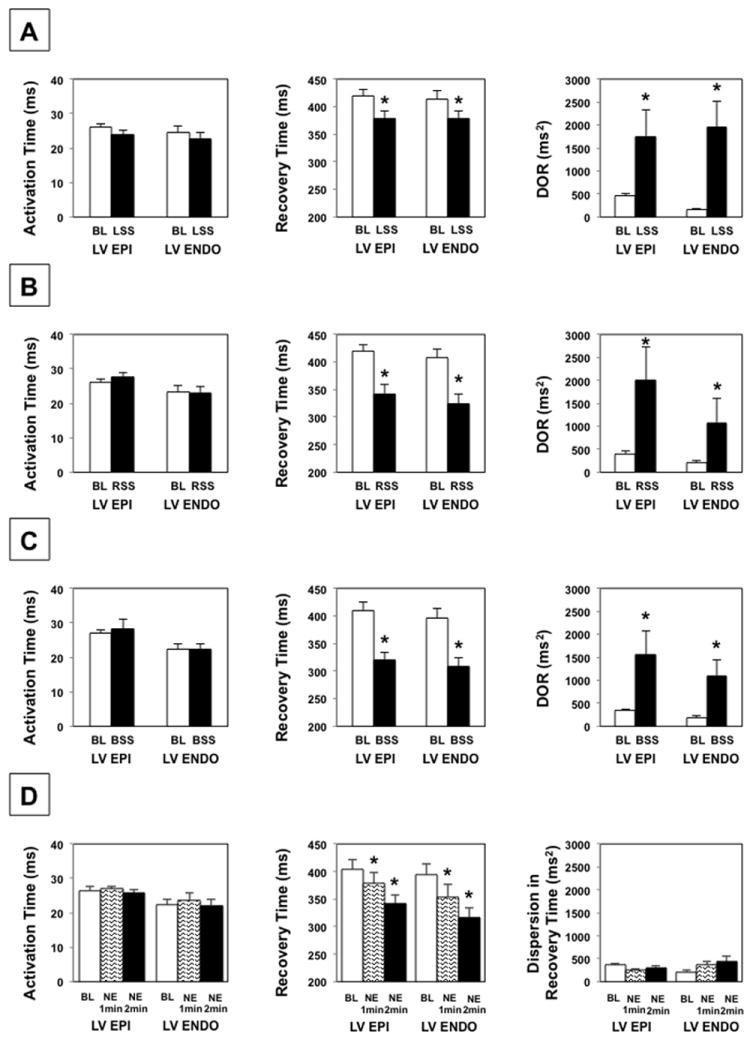
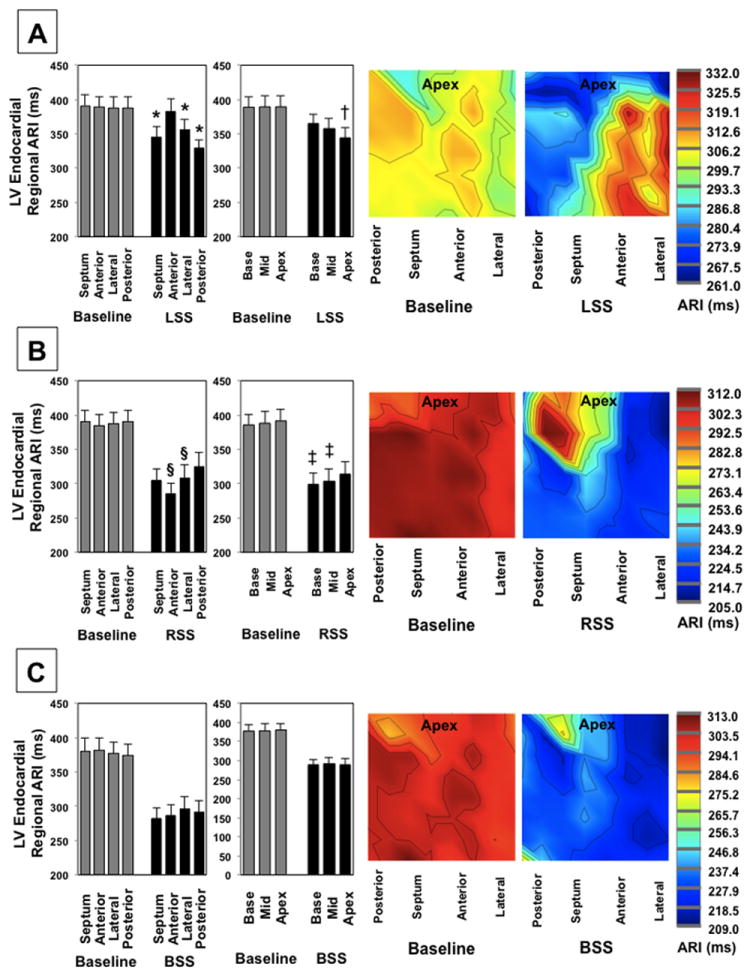
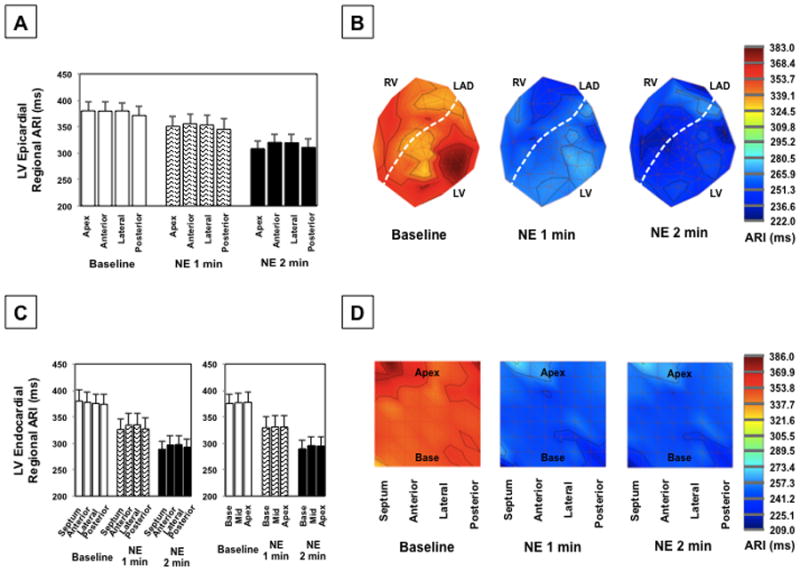
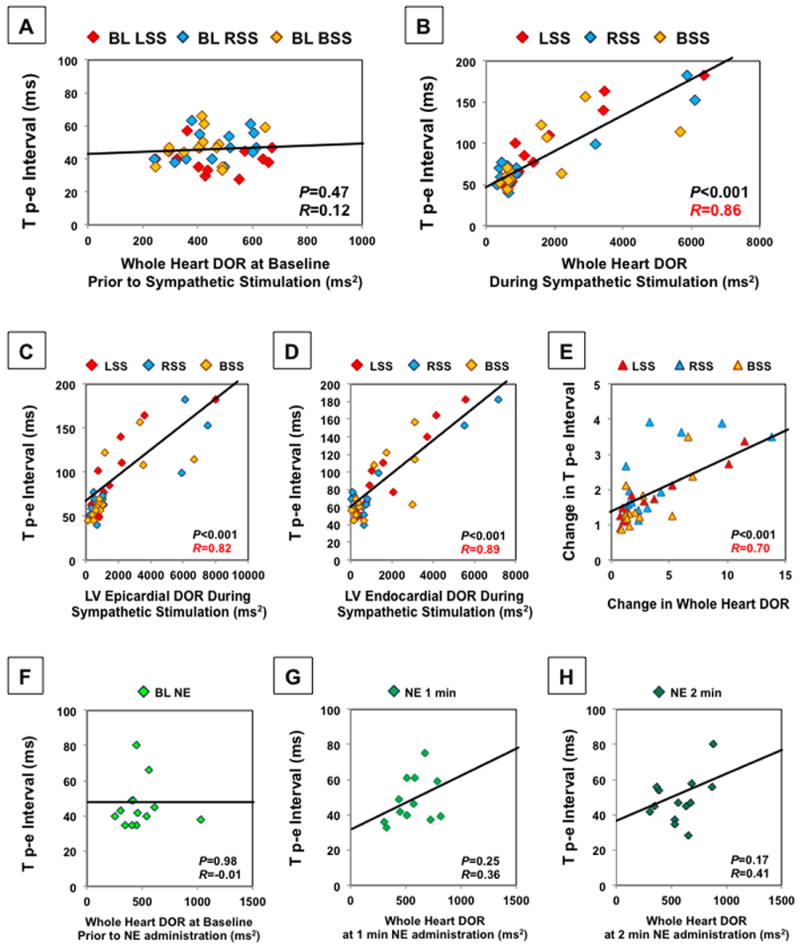
Methods and results: In Yorkshire pigs (n=13), a sternotomy was performed and the heart and bilateral stellate ganglia were exposed. A 56-electrode sock and 64-electrode basket catheter were placed around the epicardium and in the left ventricle (LV), respectively. Activation recovery interval, DOR, defined as variance in repolarization time, and Tp-e were assessed before and after left, right, and bilateral stellate ganglia stimulation and norepinephrine infusion. LV endocardial and epicardial activation recovery intervals significantly decreased, and LV endocardial and epicardial DOR increased during sympathetic nerve stimulation. There were no LV epicardial versus endocardial differences in activation recovery interval during sympathetic stimulation, and regional endocardial activation recovery interval patterns were similar to the epicardium. Tp-e prolonged during left (from 40.4±2.2 ms to 92.4±12.4 ms; P<0.01), right (from 47.7±2.6 ms to 80.7±11.5 ms; P<0.01), and bilateral (from 47.5±2.8 ms to 78.1±9.8 ms; P<0.01) stellate stimulation and strongly correlated with whole heart DOR during stimulation (P<0.001, R=0.86). Of note, norepinephrine infusion did not increase DOR or Tp-e.
Conclusions: Regional patterns of LV endocardial sympathetic innervation are similar to that of LV epicardium. Tp-e correlated with whole heart DOR during sympathetic nerve activation. Circulating norepinephrine did not affect DOR or Tp-e.
Keywords: ECG; T wave; action potential; autonomic nervous system; dispersion; sympathetic.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures




References
-
- Zhou S, Jung BC, Tan AY, Trang VQ, Gholmieh G, Han SW, Lin SF, Fishbein MC, Chen PS, Chen LS. Spontaneous stellate ganglion nerve activity and ventricular arrhythmia in a canine model of sudden death. Heart Rhythm. 2008;5:131–139. - PubMed
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Bourke T, Vaseghi M, Michowitz Y, Sankhla V, Shah M, Swapna N, Boyle NG, Mahajan A, Narasimhan C, Lokhandwala Y, Shivkumar K. Neuraxial modulation for refractory ventricular arrhythmias: Value of thoracic epidural anesthesia and surgical left cardiac sympathetic denervation. Circulation. 2010;121:2255–2262. - PMC - PubMed
-
- Schwartz PJ, Locati EH, Moss AJ, Crampton RS, Trazzi R, Ruberti U. Left cardiac sympathetic denervation in the therapy of congenital long qt syndrome. A worldwide report. Circulation. 1991;84:503–511. - PubMed
