

Combined MYC and P53 defects emerge at medulloblastoma relapse and define rapidly progressive, therapeutically targetable disease
- PMID: 25533335
- PMCID: PMC4297293
- DOI: 10.1016/j.ccell.2014.11.002
Combined MYC and P53 defects emerge at medulloblastoma relapse and define rapidly progressive, therapeutically targetable disease
Abstract
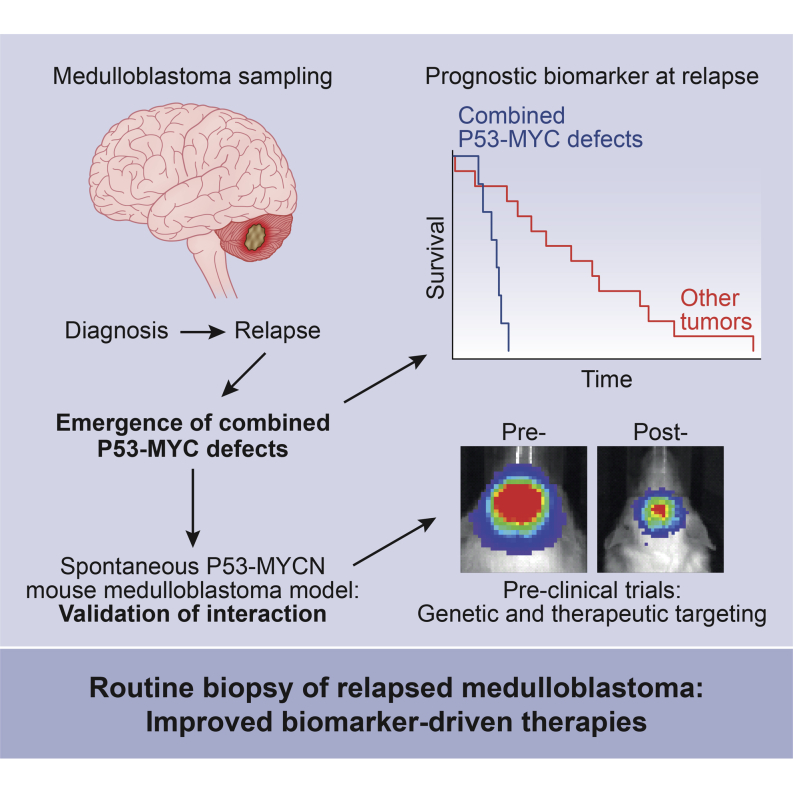
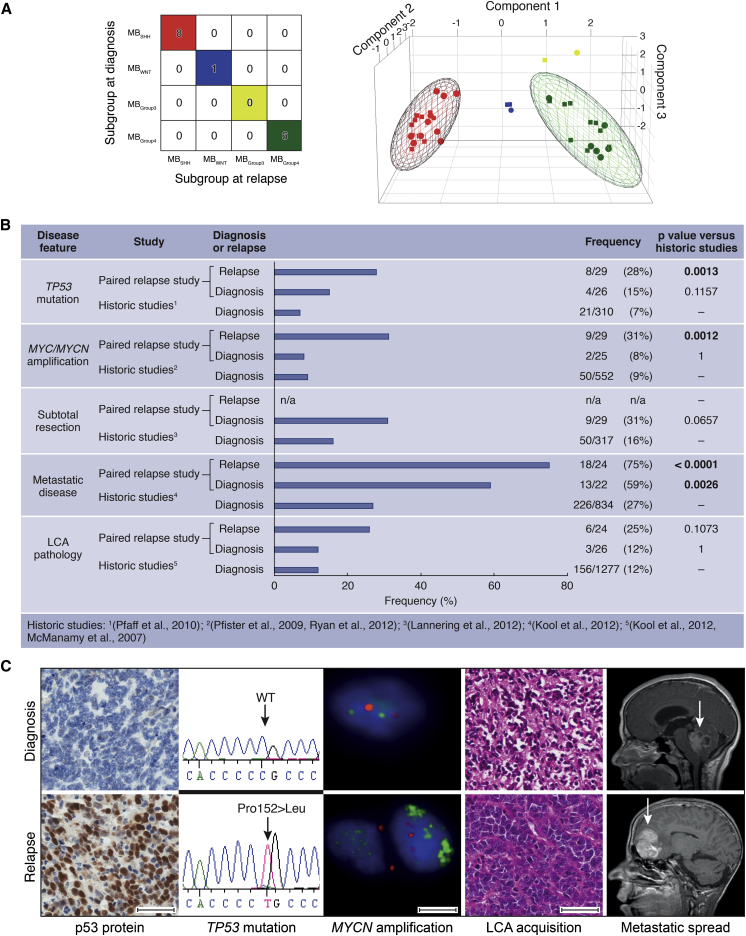
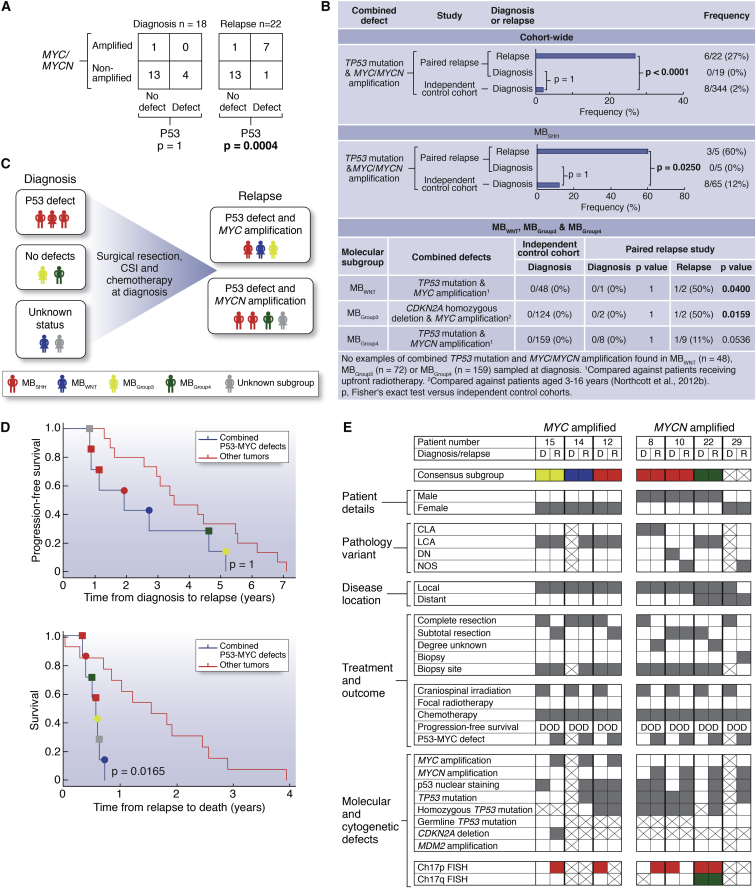
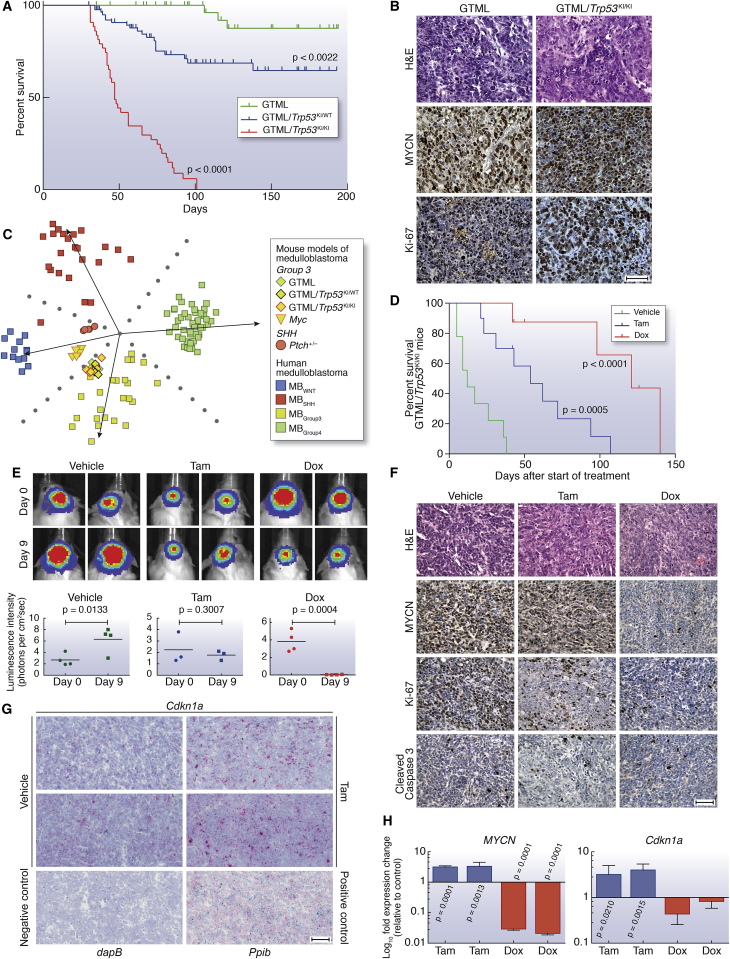
We undertook a comprehensive clinical and biological investigation of serial medulloblastoma biopsies obtained at diagnosis and relapse. Combined MYC family amplifications and P53 pathway defects commonly emerged at relapse, and all patients in this group died of rapidly progressive disease postrelapse. To study this interaction, we investigated a transgenic model of MYCN-driven medulloblastoma and found spontaneous development of Trp53 inactivating mutations. Abrogation of p53 function in this model produced aggressive tumors that mimicked characteristics of relapsed human tumors with combined P53-MYC dysfunction. Restoration of p53 activity and genetic and therapeutic suppression of MYCN all reduced tumor growth and prolonged survival. Our findings identify P53-MYC interactions at medulloblastoma relapse as biomarkers of clinically aggressive disease that may be targeted therapeutically.
Copyright © 2015 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Abdi H. Bonferroni and Sidak corrections for multiple comparisons. In: Salkind N.J., editor. Encyclopedia of Measurement and Statistics. Sage; Thousand Oaks, CA: 2007.
-
- Berggren P., Kumar R., Sakano S., Hemminki L., Wada T., Steineck G., Adolfsson J., Larsson P., Norming U., Wijkstrom H., Hemminki K. Detecting homozygous deletions in the CDKN2A(p16(INK4a))/ARF(p14(ARF)) gene in urinary bladder cancer using real-time quantitative PCR. Clin. Cancer Res. 2003;9:235–242. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
