

A practical approach to imaging the axilla
- PMID: 25534139
- PMCID: PMC4376818
- DOI: 10.1007/s13244-014-0367-8
A practical approach to imaging the axilla
Abstract
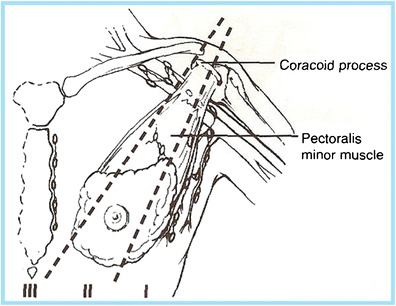
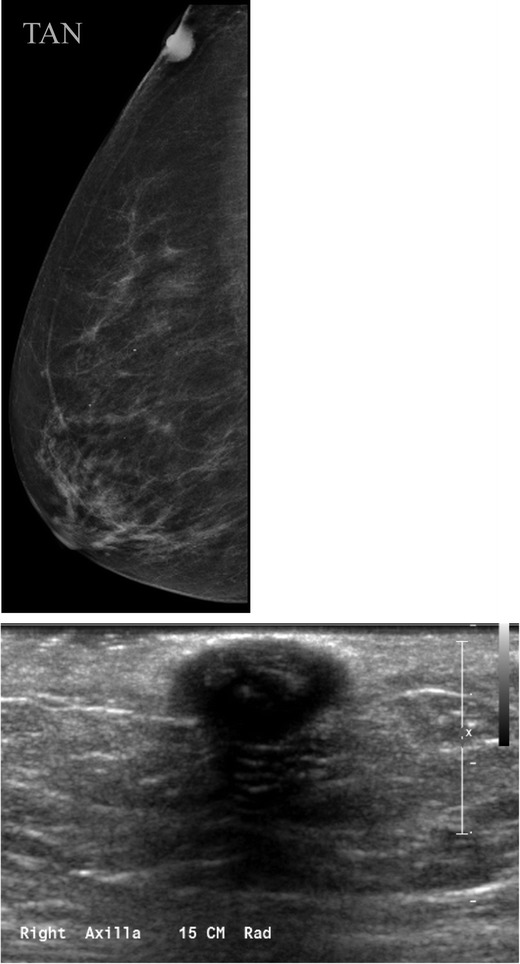
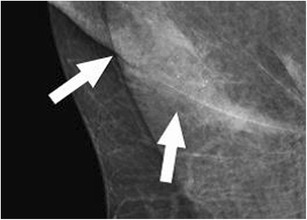
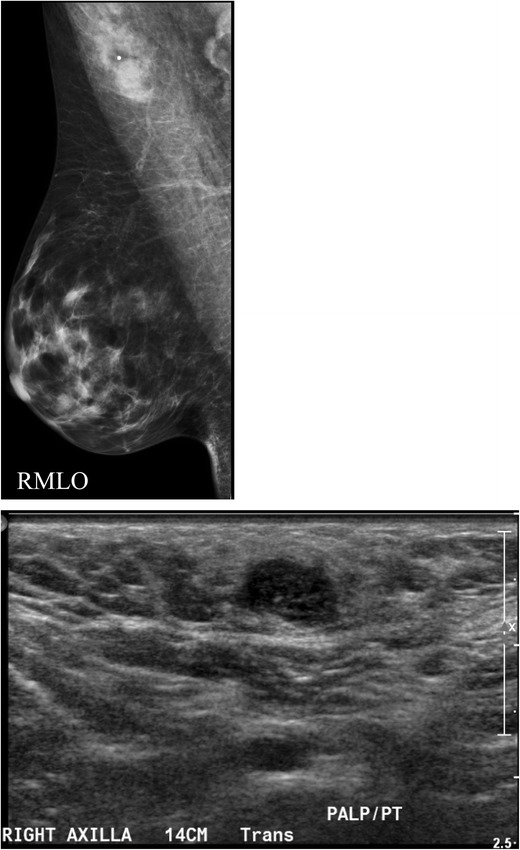
Imaging of the axilla typically occurs when patients present with axillary symptoms or newly diagnosed breast cancer. An awareness of the axillary anatomy is essential in order to generate an accurate differential diagnosis and guide patient management. The purpose of this article is to review the indications for axillary imaging, discuss the logistics of the scanning technique and percutaneous interventions, and present the imaging findings and management of a variety of breast diseases involving the axilla. Teaching points • Knowledge of normal axillary anatomy aids in determining the aetiology of an axillary mass. • The differential diagnosis of an axillary mass is broad and can be subdivided by the location of the lesion. • Imaging evaluation of the axilla usually entails diagnostic mammography and targeted ultrasound. • FNA or core needle biopsies are safe and accurate methods for diagnosis and guiding management.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
