

Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: a randomized clinical trial
- PMID: 25536254
- PMCID: PMC4335311
- DOI: 10.1001/jama.2014.16058
Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: a randomized clinical trial
Abstract
Importance: Hypothermia at 33.5°C for 72 hours for neonatal hypoxic ischemic encephalopathy reduces death or disability to 44% to 55%; longer cooling and deeper cooling are neuroprotective in animal models.
Objective: To determine if longer duration cooling (120 hours), deeper cooling (32.0°C), or both are superior to cooling at 33.5°C for 72 hours in neonates who are full-term with moderate or severe hypoxic ischemic encephalopathy.
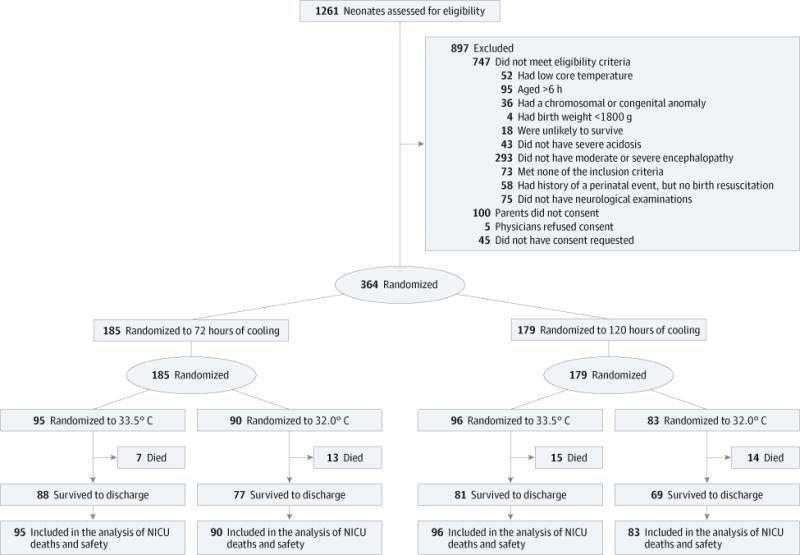
Design, setting, and participants: A randomized, 2 × 2 factorial design clinical trial performed in 18 US centers in the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Neonatal Research Network between October 2010 and November 2013.
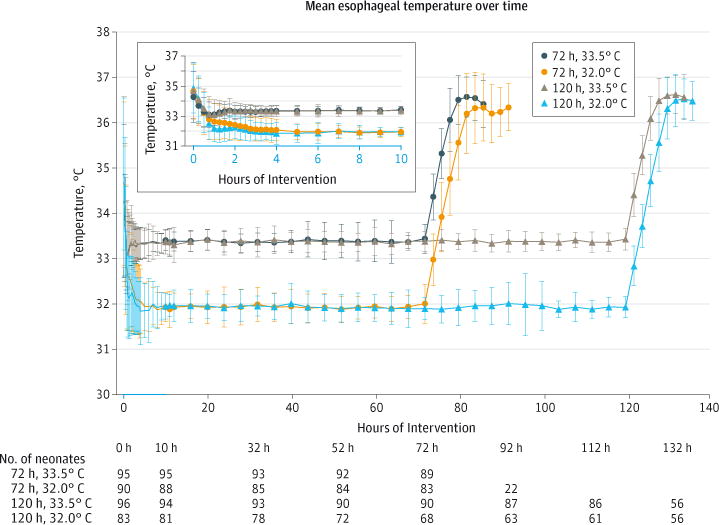
Interventions: Neonates were assigned to 4 hypothermia groups; 33.5°C for 72 hours, 32.0°C for 72 hours, 33.5°C for 120 hours, and 32.0°C for 120 hours.
Main outcomes and measures: The primary outcome of death or disability at 18 to 22 months is ongoing. The independent data and safety monitoring committee paused the trial to evaluate safety (cardiac arrhythmia, persistent acidosis, major vessel thrombosis and bleeding, and death in the neonatal intensive care unit [NICU]) after the first 50 neonates were enrolled, then after every subsequent 25 neonates. The trial was closed for emerging safety profile and futility analysis after the eighth review with 364 neonates enrolled (of 726 planned). This report focuses on safety and NICU deaths by marginal comparisons of 72 hours' vs 120 hours' duration and 33.5°C depth vs 32.0°C depth (predefined secondary outcomes).
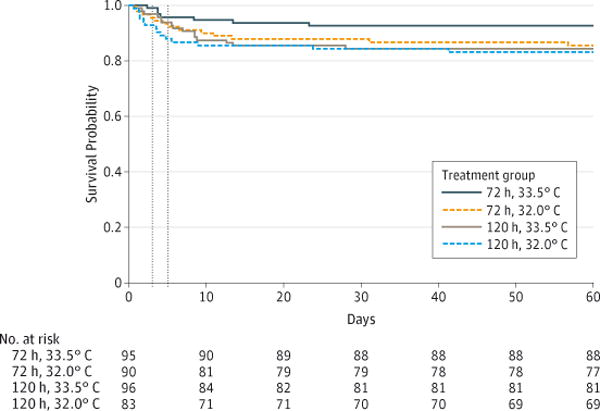
Results: The NICU death rates were 7 of 95 neonates (7%) for the 33.5°C for 72 hours group, 13 of 90 neonates (14%) for the 32.0°C for 72 hours group, 15 of 96 neonates (16%) for the 33.5°C for 120 hours group, and 14 of 83 neonates (17%) for the 32.0°C for 120 hours group. The adjusted risk ratio (RR) for NICU deaths for the 120 hours group vs 72 hours group was 1.37 (95% CI, 0.92-2.04) and for the 32.0°C group vs 33.5°C group was 1.24 (95% CI, 0.69-2.25). Safety outcomes were similar between the 120 hours group vs 72 hours group and the 32.0°C group vs 33.5°C group, except major bleeding occurred among 1% in the 120 hours group vs 3% in the 72 hours group (RR, 0.25 [95% CI, 0.07-0.91]). Futility analysis determined that the probability of detecting a statistically significant benefit for longer cooling, deeper cooling, or both for NICU death was less than 2%.
Conclusions and relevance: Among neonates who were full-term with moderate or severe hypoxic ischemic encephalopathy, longer cooling, deeper cooling, or both compared with hypothermia at 33.5°C for 72 hours did not reduce NICU death. These results have implications for patient care and design of future trials.
Trial registration: clinicaltrials.gov Identifier: NCT01192776.
Figures
Comment in
-
Depth and duration of cooling for perinatal asphyxial encephalopathy.JAMA. 2014 Dec 24-31;312(24):2623-4. doi: 10.1001/jama.2014.15959. JAMA. 2014. PMID: 25536251 No abstract available.
-
Longer and deeper cooling for hypoxic ischemic encephalopathy in neonates does not reduce mortality.Acta Paediatr. 2017 Jul;106(7):1200. doi: 10.1111/apa.13781. Epub 2017 Mar 12. Acta Paediatr. 2017. PMID: 28295535 No abstract available.
References
-
- Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy. Lancet. 2005;365(9460):663–670. - PubMed
-
- Shankaran S, Laptook AR, Ehrenkranz RA, et al. National Institute of Child Health and Human Development Neonatal Research Network Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353(15):1574–1584. - PubMed
-
- Azzopardi DV, Strohm B, Edwards AD, et al. TOBY Study Group Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med. 2009;361(14):1349–1358. - PubMed
-
- Simbruner G, Mittal RA, Rohlmann F, Muche R, neo.nEURO.network Trial Participants Systemic hypothermia after neonatal encephalopathy. Pediatrics. 2010;126(4):e771–e778. - PubMed
-
- Jacobs SE, Morley CJ, Inder TE, et al. Infant Cooling Evaluation Collaboration Whole-body hypothermia for term and near-term newborns with hypoxic-ischemic encephalopathy. Arch Pediatr Adolesc Med. 2011;165(8):692–700. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HD021385/HD/NICHD NIH HHS/United States
- UL1 TR77/TR/NCATS NIH HHS/United States
- U10 HD68278/HD/NICHD NIH HHS/United States
- UG1 HD068270/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- U10 HD53089/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- U10 HD27853/HD/NICHD NIH HHS/United States
- U10 HD068270/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- U10 HD068284/HD/NICHD NIH HHS/United States
- M01 RR32/RR/NCRR NIH HHS/United States
- UL1 RR24128/RR/NCRR NIH HHS/United States
- U10 HD27851/HD/NICHD NIH HHS/United States
- UL1 TR442/TR/NCATS NIH HHS/United States
- U10 HD68284/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD40689/HD/NICHD NIH HHS/United States
- UL1 TR93/TR/NCATS NIH HHS/United States
- U10 HD40492/HD/NICHD NIH HHS/United States
- U10 HD21364/HD/NICHD NIH HHS/United States
- U10 HD34216/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UL1 TR6/TR/NCATS NIH HHS/United States
- UL1 TR41/TR/NCATS NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- M01 RR70/RR/NCRR NIH HHS/United States
- U10 HD36790/HD/NICHD NIH HHS/United States
- U10 HD27880/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- U10 HD27904/HD/NICHD NIH HHS/United States
- M01 RR633/RR/NCRR NIH HHS/United States
- U10 HD53109/HD/NICHD NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD068244/HD/NICHD NIH HHS/United States
- U10 HD27856/HD/NICHD NIH HHS/United States
- U10 HD068263/HD/NICHD NIH HHS/United States
- U10 HD68263/HD/NICHD NIH HHS/United States
- UL1 TR000142/TR/NCATS NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- M01 RR80/RR/NCRR NIH HHS/United States
- U10 HD68270/HD/NICHD NIH HHS/United States
- U10 HD68244/HD/NICHD NIH HHS/United States
- U10 HD21373/HD/NICHD NIH HHS/United States
- U10 HD21385/HD/NICHD NIH HHS/United States
- UL1 TR454/TR/NCATS NIH HHS/United States
- UL1 TR000371/TR/NCATS NIH HHS/United States
- UL1 TR42/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
