

A phase I dose escalation trial of MAGE-A3- and HPV16-specific peptide immunomodulatory vaccines in patients with recurrent/metastatic (RM) squamous cell carcinoma of the head and neck (SCCHN)
- PMID: 25537079
- PMCID: PMC4381442
- DOI: 10.1007/s00262-014-1640-x
A phase I dose escalation trial of MAGE-A3- and HPV16-specific peptide immunomodulatory vaccines in patients with recurrent/metastatic (RM) squamous cell carcinoma of the head and neck (SCCHN)
Abstract
Background: We conducted a phase I dose escalation study to evaluate the safety and immunologic response to peptide immunomodulatory vaccines GL-0810 (HPV16) and GL-0817 (MAGE-A3) in HPV16 and MAGE-A3-positive RM-SCCHN patients, respectively.
Methods: Three dose levels (500, 1,000, and 1,500 µg) of GL-0810 or GL-0817 with adjuvants Montanide (1.2 ml) and GM-CSF (100 µg/m2) were administered subcutaneously q2 weeks for a total of four vaccinations in HPV16 and MAGE-A3-positive RM-SCCHN patients, respectively.
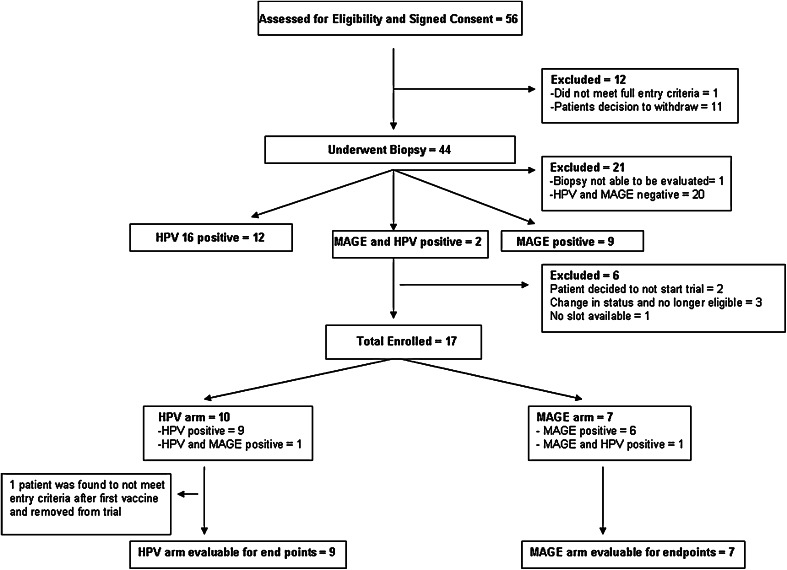
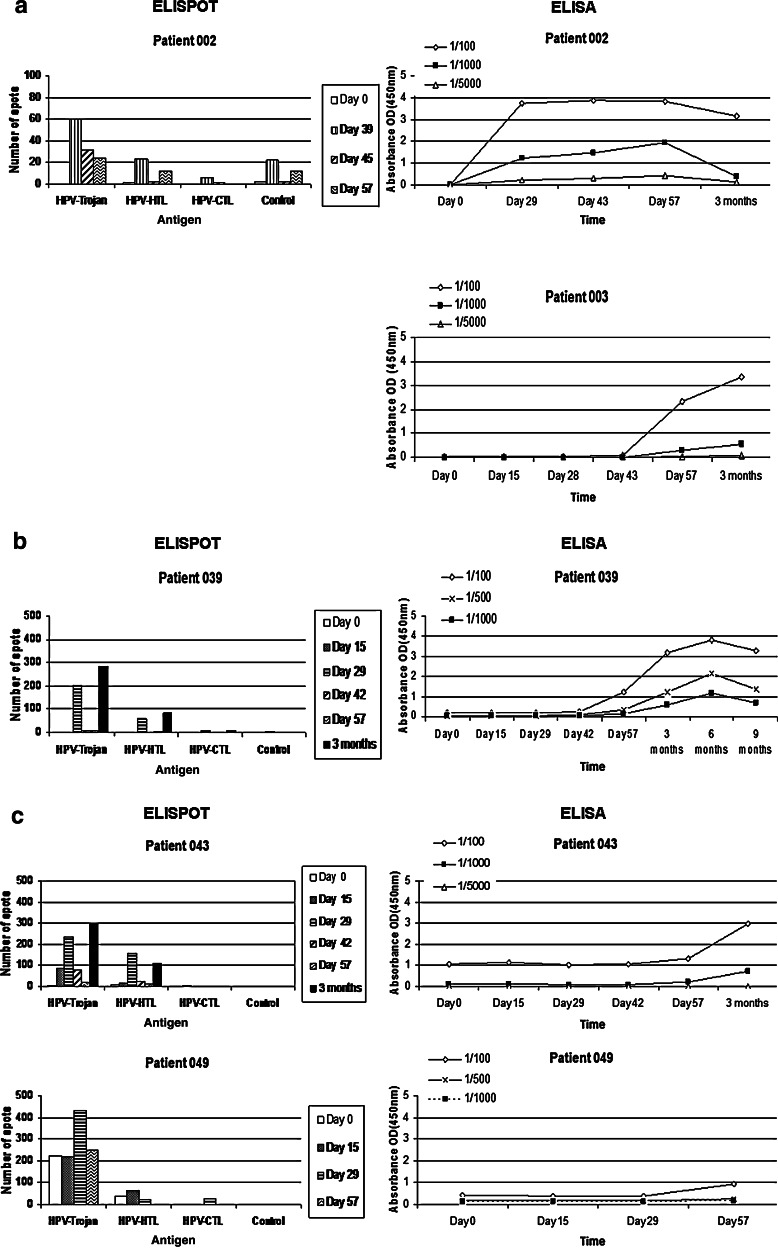
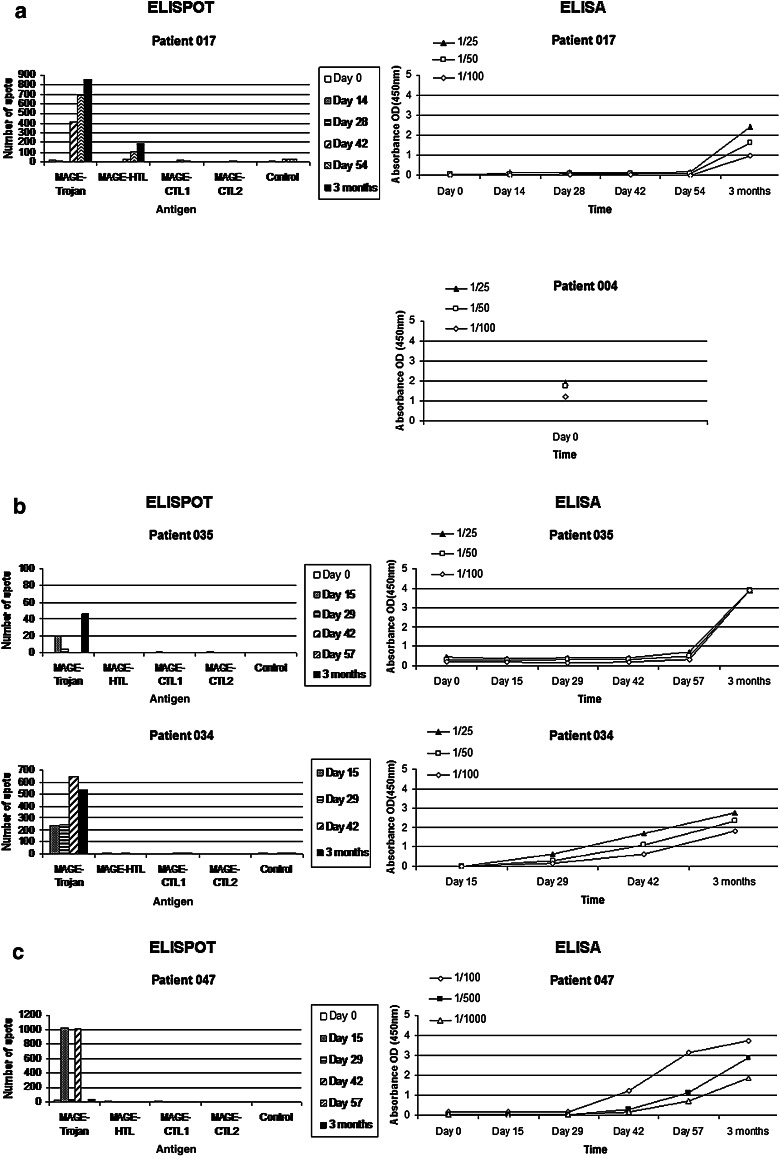
Results: Nine and seven patients were enrolled in the HPV16 and MAGE-A3 cohorts, respectively. No dose-limiting toxicities were observed, and toxicity was predominantly local and grade 1 (erythema, pain, and itching at the injection site). In those patients who received all four vaccinations, 80 % (4/5) of the HPV16 cohort and 67 % (4/6) of the MAGE-A3 cohort developed antigen-specific T cell and antibody responses to the vaccine. Significant concordance between T cell and antibody responses was observed for both groups. No clear dose-response correlation was seen. All patients progressed by RECIST at first repeat imaging, except for one patient in the MAGE-A3 500 µg cohort who had stable disease for 10.5 months. The median PFS and OS for the MAGE-A3 cohorts were 79 and 183 days, respectively, and for the HPV16 cohort 80 and 196 days, respectively.
Conclusions: GL-0810 and GL-0817 were well tolerated in patients with RM-SCCHN with T cell and antibody responses observed in the majority of patients who received all four vaccinations.
Figures
Similar articles
-
Induction of MAGE-A3 and HPV-16 immunity by Trojan vaccines in patients with head and neck carcinoma.Head Neck. 2012 Dec;34(12):1734-46. doi: 10.1002/hed.22004. Epub 2012 Jan 27. Head Neck. 2012. PMID: 22287423 Free PMC article.
-
Combination immunotherapy after ASCT for multiple myeloma using MAGE-A3/Poly-ICLC immunizations followed by adoptive transfer of vaccine-primed and costimulated autologous T cells.Clin Cancer Res. 2014 Mar 1;20(5):1355-65. doi: 10.1158/1078-0432.CCR-13-2817. Epub 2014 Feb 11. Clin Cancer Res. 2014. PMID: 24520093 Free PMC article. Clinical Trial.
-
Characterization of preexisting MAGE-A3-specific CD4+ T cells in cancer patients and healthy individuals and their activation by protein vaccination.J Immunol. 2009 Oct 1;183(7):4800-8. doi: 10.4049/jimmunol.0900903. Epub 2009 Sep 4. J Immunol. 2009. PMID: 19734225
-
Melanoma-associated antigen-A3 vaccination in the treatment of non-small-cell lung cancer.Expert Opin Biol Ther. 2014 Mar;14(3):365-76. doi: 10.1517/14712598.2014.880421. Epub 2014 Jan 24. Expert Opin Biol Ther. 2014. PMID: 24456101 Review.
-
[Future Prospects on neoplasm antigen vaccine therapy for patients with head and neck squamous cell carcinoma].Nihon Jibiinkoka Gakkai Kaiho. 2002 Mar;105(3):201-7. Nihon Jibiinkoka Gakkai Kaiho. 2002. PMID: 12014346 Review. Japanese. No abstract available.
Cited by
-
Current status and perspective of tumor immunotherapy for head and neck squamous cell carcinoma.Front Cell Dev Biol. 2022 Aug 26;10:941750. doi: 10.3389/fcell.2022.941750. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36092724 Free PMC article. Review.
-
Cancer Vaccines: Adjuvant Potency, Importance of Age, Lifestyle, and Treatments.Front Immunol. 2021 Feb 17;11:615240. doi: 10.3389/fimmu.2020.615240. eCollection 2020. Front Immunol. 2021. PMID: 33679703 Free PMC article. Review.
-
Enhancement of HPV therapeutic peptide-based vaccine efficacy through combination therapies and improved delivery strategies: A review.Hum Vaccin Immunother. 2024 Dec 31;20(1):2396710. doi: 10.1080/21645515.2024.2396710. Epub 2024 Aug 28. Hum Vaccin Immunother. 2024. PMID: 39193781 Free PMC article. Review.
-
Targeted Therapy in Oropharyngeal Squamous Cell Carcinoma: The Implications of HPV for Therapy.Rare Cancers Ther. 2015;3(1):89-117. doi: 10.1007/s40487-015-0008-5. Epub 2015 Sep 9. Rare Cancers Ther. 2015. PMID: 27182480 Free PMC article. Review.
-
Immunotherapy in head and neck squamous cell carcinoma: a narrative review.Front Oral Maxillofac Med. 2022 Sep;4:28. doi: 10.21037/fomm-21-48. Epub 2022 Sep 10. Front Oral Maxillofac Med. 2022. PMID: 36105623 Free PMC article.
References
-
- McDonald MW, Lawson J, Garg MK, et al. ACR appropriateness criteria retreatment of recurrent head and neck cancer after prior definitive radiation expert panel on radiation oncology-head and neck cancer. Int J Radiat Oncol Biol Phys. 2011;80:1292–1298. doi: 10.1016/j.ijrobp.2011.02.014. - DOI - PubMed
-
- Vermorken JB, Specenier P (2010) Optimal treatment for recurrent/metastatic head and neck cancer. Ann Oncol 21 Suppl 7: vii252–261. doi 10.1093/annonc/mdq453 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
