

Placental growth factor influences maternal cardiovascular adaptation to pregnancy in mice
- PMID: 25537372
- PMCID: PMC4490891
- DOI: 10.1095/biolreprod.114.124677
Placental growth factor influences maternal cardiovascular adaptation to pregnancy in mice
Abstract
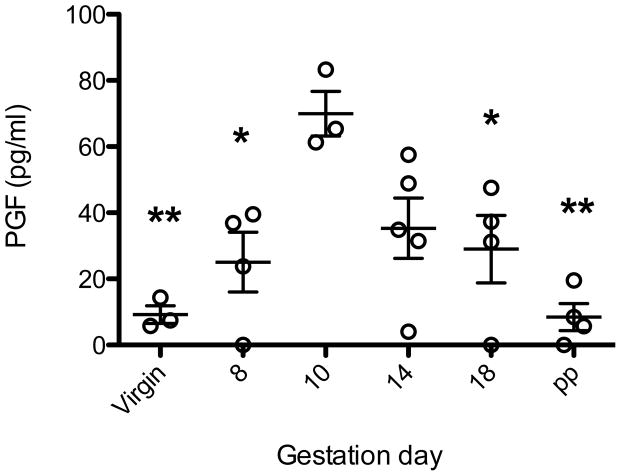
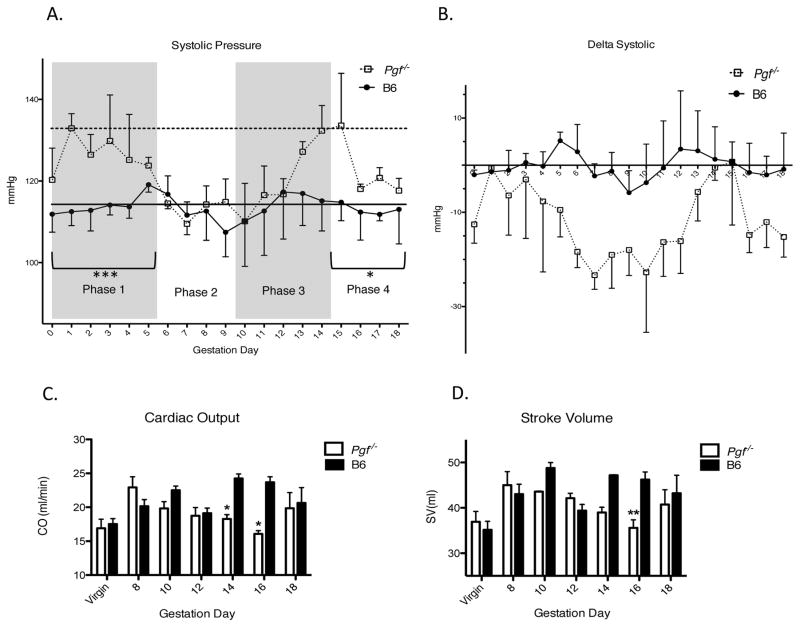
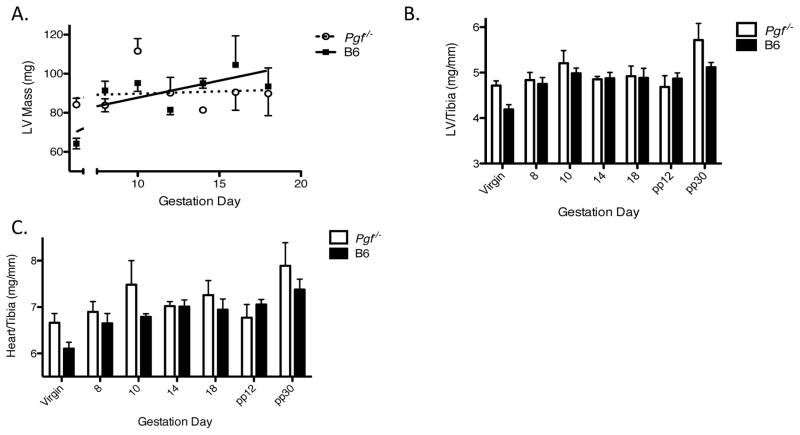
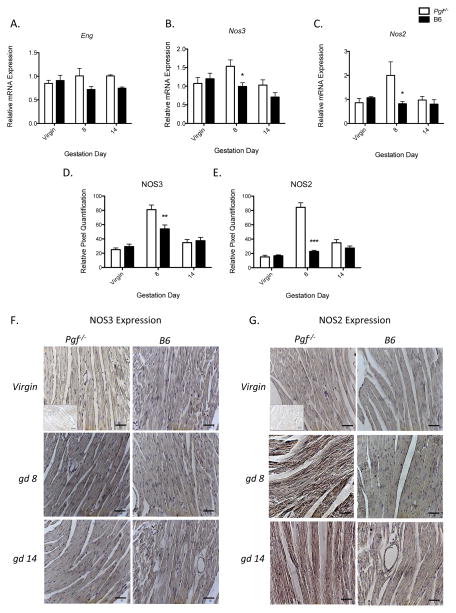
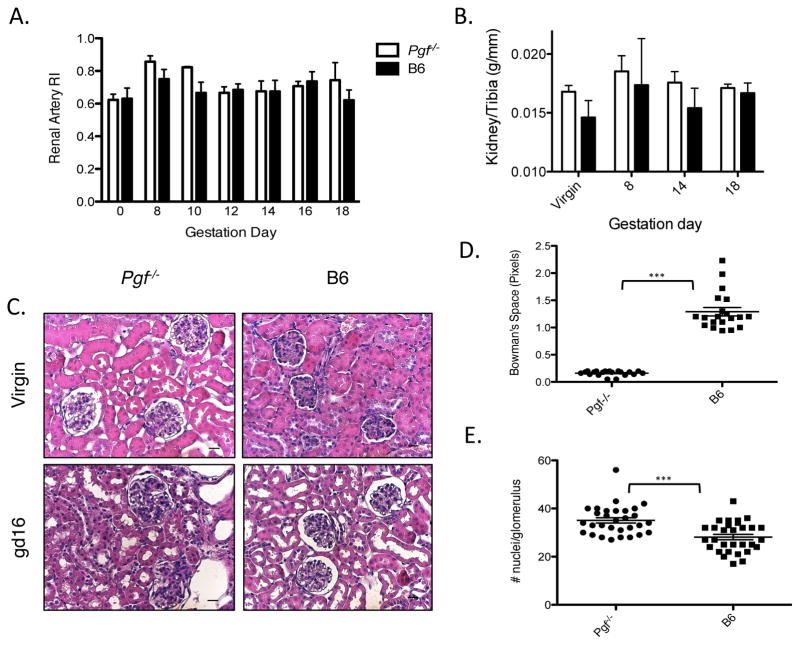
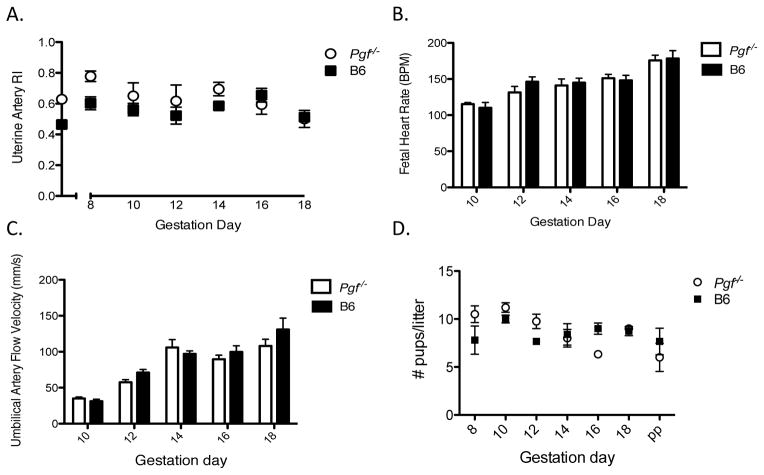
In healthy human pregnancies, placental growth factor (PGF) concentrations rise in maternal plasma during early gestation, peak over Weeks 26-30, then decline. Because PGF in nongravid subjects participates in protection against and recovery from cardiac pathologies, we asked if PGF contributes to pregnancy-induced maternal cardiovascular adaptations. Cardiovascular function and structure were evaluated in virgin, pregnant, and postpartum C56BL/6-Pgf(-) (/) (-) (Pgf(-) (/) (-)) and C57BL/6-Pgf(+/+) (B6) mice using plethysmography, ultrasound, quantitative PCR, and cardiac and renal histology. Pgf(-/-) females had higher systolic blood pressure in early and late pregnancy but an extended, abnormal midpregnancy interval of depressed systolic pressure. Pgf(-/-) cardiac output was lower than gestation day (gd)-matched B6 after midpregnancy. While Pgf(-) (/) (-) left ventricular mass was greater than B6, only B6 showed the expected gestational gain in left ventricular mass. Expression of vasoactive genes in the left ventricle differed at gd8 with elevated Nos expression in Pgf(-) (/) (-) but not at gd14. By gd16, Pgf(-) (/) (-) kidneys were hypertrophic and had glomerular pathology. This study documents for the first time that PGF is associated with the systemic maternal cardiovascular adaptations to pregnancy.
Keywords: cardiac remodeling; cardiovascular risk; fetal growth; placenta; ultrasound.
© 2015 by the Society for the Study of Reproduction, Inc.
Conflict of interest statement
Peter Carmeliet holds patents on the use PGF as a cardioprotectant.
Figures
References
-
- Vrachnis N, Kalampokas E, Sifakis S, Vitoratos N, Kalampokas T, Botsis D, Iliodromiti Z. Placental growth factor (PlGF): a key to optimizing fetal growth. J Matern Fetal Neonatal Med. 2013;26:995–1002. - PubMed
-
- Carnevale D, Lembo G. Placental growth factor and cardiac inflammation. Trends Cardiovasc Med. 2012;22:209–212. - PubMed
-
- Luttun A, Tjwa M, Carmeliet P. Placental growth factor (PlGF) and its receptor Flt-1 (VEGFR-1): novel therapeutic targets for angiogenic disorders. Ann N Y Acad Sci. 2002;979:80–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
