

Therapies for the bone in mucopolysaccharidoses
- PMID: 25537451
- PMCID: PMC4312706
- DOI: 10.1016/j.ymgme.2014.12.001
Therapies for the bone in mucopolysaccharidoses
Abstract
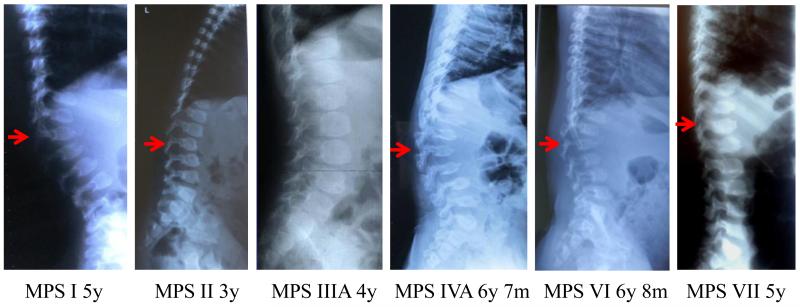
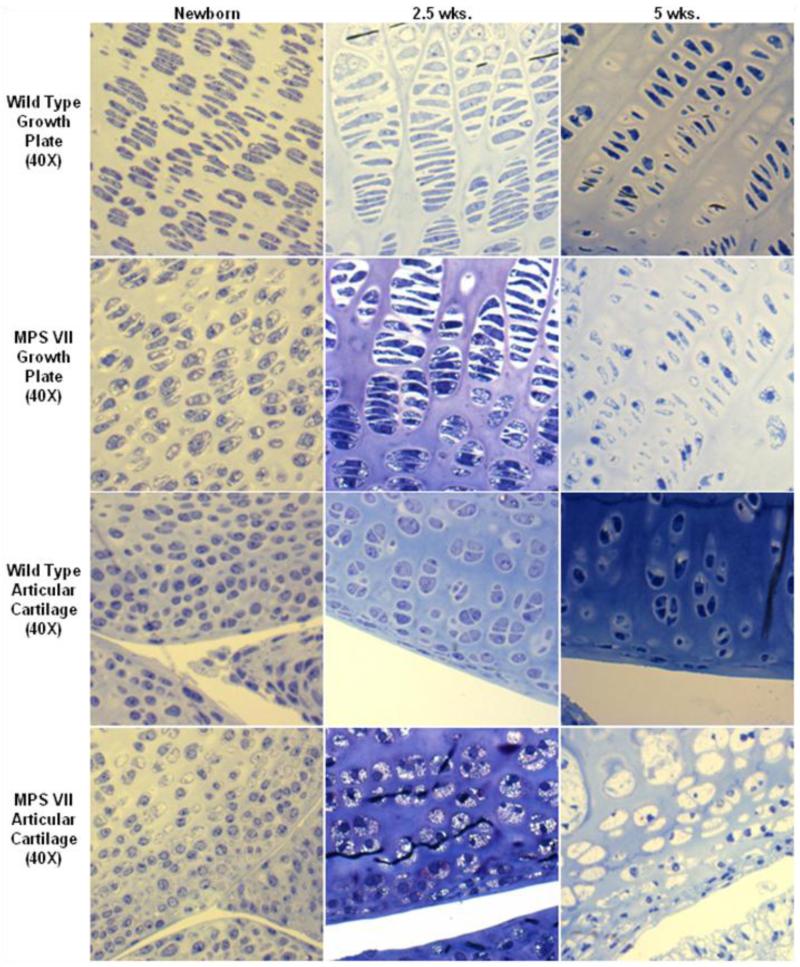
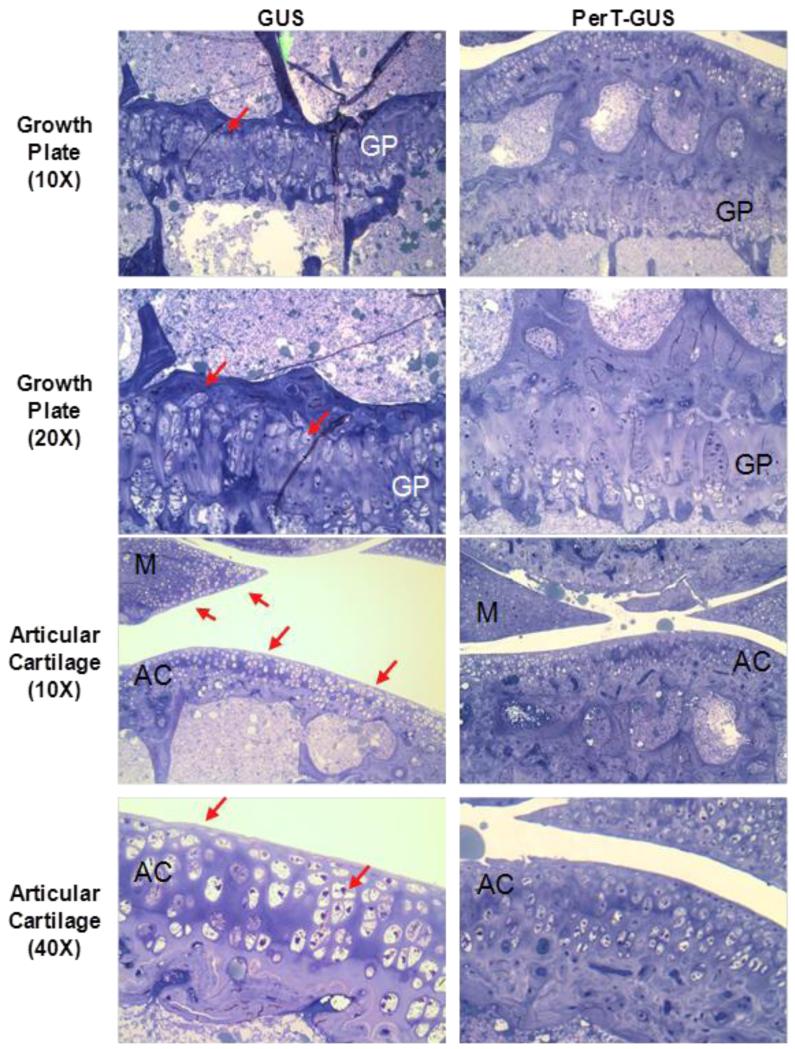
Patients with mucopolysaccharidoses (MPS) have accumulation of glycosaminoglycans in multiple tissues which may cause coarse facial features, mental retardation, recurrent ear and nose infections, inguinal and umbilical hernias, hepatosplenomegaly, and skeletal deformities. Clinical features related to bone lesions may include marked short stature, cervical stenosis, pectus carinatum, small lungs, joint rigidity (but laxity for MPS IV), kyphoscoliosis, lumbar gibbus, and genu valgum. Patients with MPS are often wheelchair-bound and physical handicaps increase with age as a result of progressive skeletal dysplasia, abnormal joint mobility, and osteoarthritis, leading to 1) stenosis of the upper cervical region, 2) restrictive small lung, 3) hip dysplasia, 4) restriction of joint movement, and 5) surgical complications. Patients often need multiple orthopedic procedures including cervical decompression and fusion, carpal tunnel release, hip reconstruction and replacement, and femoral or tibial osteotomy through their lifetime. Current measures to intervene in bone disease progression are not perfect and palliative, and improved therapies are urgently required. Enzyme replacement therapy (ERT), hematopoietic stem cell transplantation (HSCT), and gene therapy are available or in development for some types of MPS. Delivery of sufficient enzyme to bone, especially avascular cartilage, to prevent or ameliorate the devastating skeletal dysplasias remains an unmet challenge. The use of an anti-inflammatory drug is also under clinical study. Therapies should start at a very early stage prior to irreversible bone lesion, and damage since the severity of skeletal dysplasia is associated with level of activity during daily life. This review illustrates a current overview of therapies and their impact for bone lesions in MPS including ERT, HSCT, gene therapy, and anti-inflammatory drugs.
Keywords: Anti-inflammatory drug; Enzyme replacement therapy; Gene therapy; Hematopoietic stem cell transplantation; Mucopolysaccharidoses; Skeletal dysplasia.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Neufeld E, Muenzer J. The mucopolysaccharidoses. In: Scriver C, Beaudet A, Sly W, Valle D, editors. The Metabolic and Molecular Bases of Inherited Disease. McGraw-Hill; New York, NY: 2001. pp. 3421–3452.
-
- Tomatsu S, Montaño A, Oikawa H, Giugliani R, Harmatz P, Smith M, Orii T. Impairment of Body Growth in Mucopolysaccharidoses, In Handbook of Growth and Growth Monitoring in Health and Disease 1. Springer; New York: 2012. pp. 2091–2117.
-
- Tomatsu S, Montaño AM, Oikawa H, Smith M, Barrera L, Chinen Y, Thacker MM, Mackenzie WG, Suzuki Y, Orii T. Mucopolysaccharidosis type IVA (Morquio A disease): clinical review and current treatment. Curr. Pharm. Biotechnol. 2011;12:931–945. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
