

Prevalence of angiotensin II type 1 receptor (AT1R)-activating autoantibodies in primary aldosteronism
- PMID: 25537460
- PMCID: PMC4314451
- DOI: 10.1016/j.jash.2014.10.009
Prevalence of angiotensin II type 1 receptor (AT1R)-activating autoantibodies in primary aldosteronism
Abstract
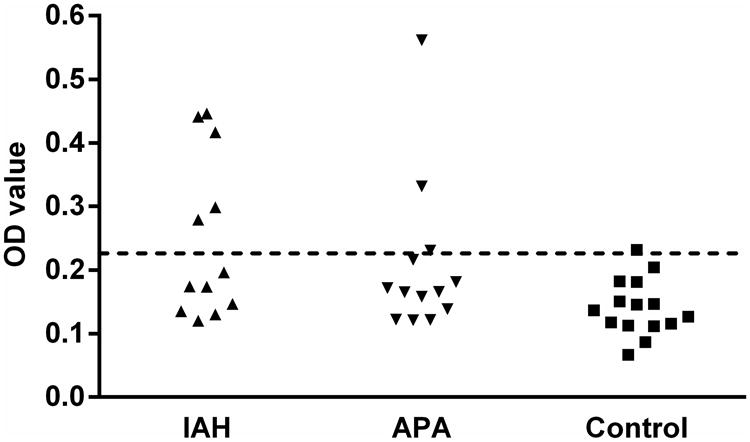
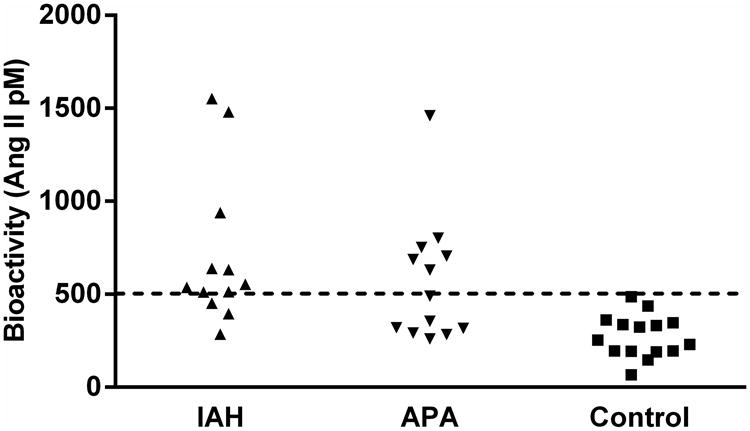
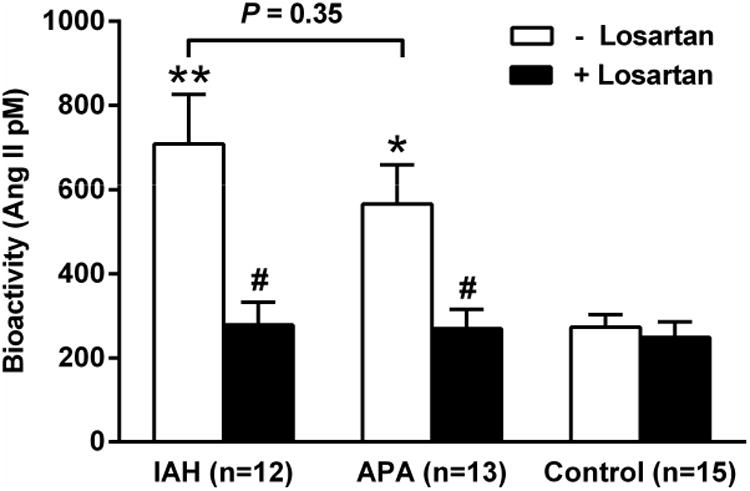
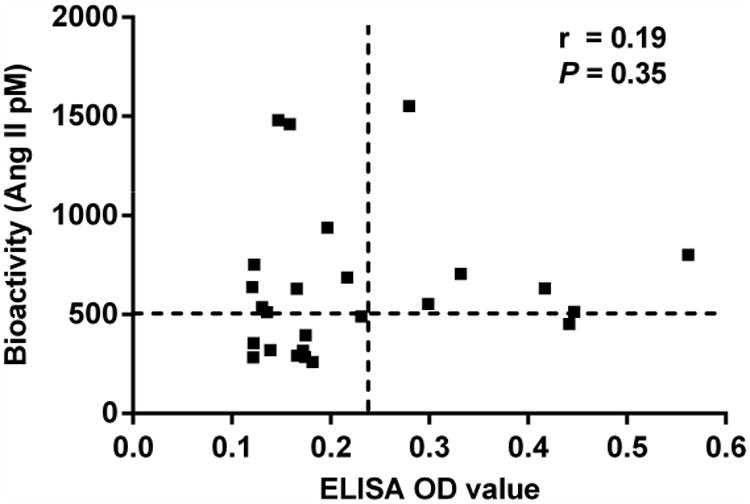
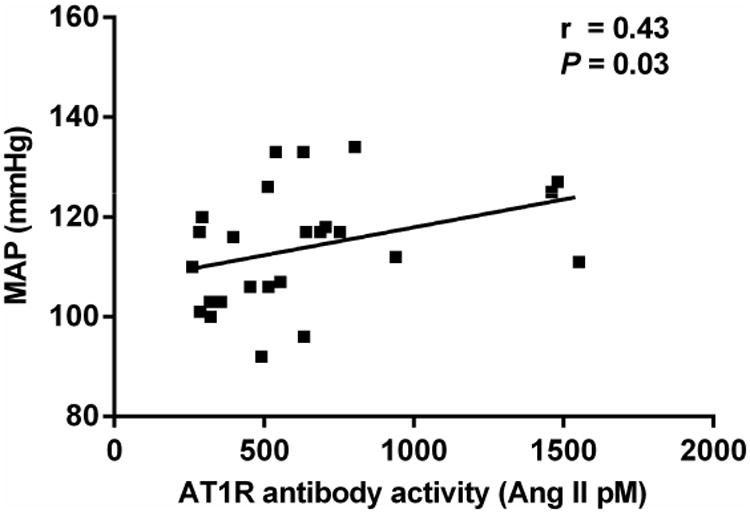
Autoantibodies to the angiotensin II type 1 receptor (AT1R) have been reported in patients with primary aldosteronism, including aldosterone producing adenoma (APA) and idiopathic adrenal hyperplasia (IAH). Sera from 25 primary aldosteronism subjects (12 with IAH and 13 with APA) and 15 normotensive control subjects were assayed for AT1R autoantibodies by enzyme-linked immunosorbent assay and an AT1R-transfected cell-based bioassay. Nine of 12 IAH subjects (75%) and six of 13 APA subjects (46%) were positive for AT1R autoantibodies in the bioactivity assay. The mean AT1R autoantibody activity for the IAH and APA subjects was significantly greater than controls (P < .001 and P < .01, respectively), and this in vitro activity was suppressed by the AT1R blocker losartan. None of the controls had significant AT1R autoantibody activity. Enzyme-linked immunosorbent assay values were less sensitive but were positive in some subjects with IAH and APA. The mean arterial pressure of these primary aldosteronism subjects correlated modestly with AT1R autoantibody activity. These data confirm the presence of active AT1R autoantibodies in a high percentage of subjects with primary aldosteronism irrespective of their underlying etiology. These observations have both pathophysiological and clinical implications.
Keywords: Aldosterone–producing adenoma; cell-based bioassay; hypertension; idiopathic adrenal hyperplasia.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: None
Figures
References
-
- Conn JW, Louis LH. Primary aldosteronism, a new clinical entity. Ann Intern Med. 1956;44:1–15. - PubMed
-
- Funder JW. The genetic basis of primary aldosteronism. Curr Hypertens Rep. 2012;14:120–4. - PubMed
-
- Azizan EA, Murthy M, Stowasser M, Gordon R, Kowalski B, Xu S, et al. Somatic mutations affecting the selectivity filter of KCNJ5 are frequent in 2 large unselected collections of adrenal aldosteronomas. Hypertension. 2012;59:587–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
