

Awareness and control of hypertension in Bangladesh: follow-up of a hypertensive cohort
- PMID: 25537780
- PMCID: PMC4275678
- DOI: 10.1136/bmjopen-2014-004983
Awareness and control of hypertension in Bangladesh: follow-up of a hypertensive cohort
Abstract
Objectives: To assess the effect of awareness and advice to seek care on blood pressure (BP) control among patients with hypertension in Bangladesh.
Design: Longitudinal study.
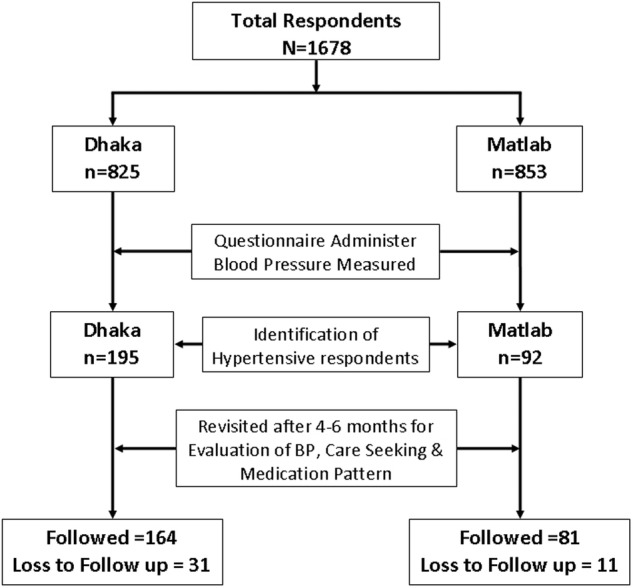
Setting: The study was carried out in icddr,b surveillance sites at rural Matlab in Chandpur district and semi-urban Kamalapur in Dhaka, Bangladesh.
Participants: Randomly selected men and non-pregnant women aged 20 years or older without any acute illness or history of any vascular events such as stroke or acute myocardial infarction.
Main outcome measure: Hypertension was defined as systolic BP (SBP) ≥140 and/or diastolic BP (DBP) ≥90 mm Hg or as self-reported hypertension under medication. We advised patients to seek care from a qualified provider and to adopt a healthy lifestyle. We compared changes in BP from baseline to follow-up at around 6 months.
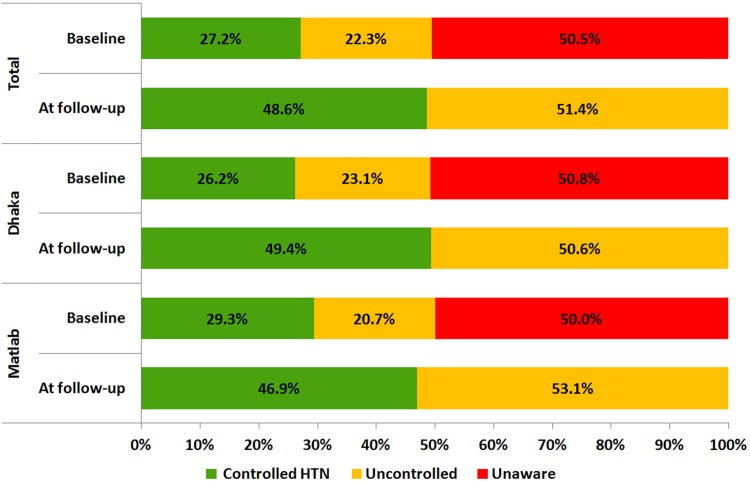
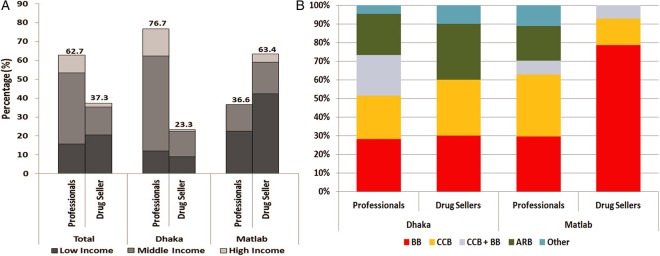
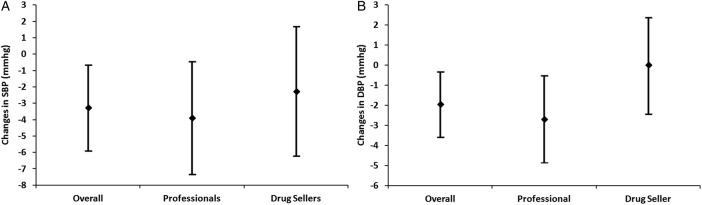
Results: Overall, 17.1% (n=287) of participants had hypertension at baseline with significantly higher prevalence in the semi-urban than in the rural population (23.6% vs 10.8%; p<0.001); half were unaware of their condition. At follow-up, 83% (n=204) reported a visit to any healthcare provider. In the semi-urban area, a higher proportion of patients visited medically qualified practitioners than in the rural area (76.7% vs 36.6%, p<0.000). SBP (-3.3±20.7 mm Hg; p<0.01) and DBP (-2.0±13.0 mm Hg; p<0.02) were lower at follow-up. Those who visited medically qualified practitioners had significant SBP (-3.9±22.4 mm Hg; p<0.03) and DBP (-2.7±14.1 mm Hg; p<0.02) reduction. BP reduction did not reach statistical significance among those visiting a pharmacist or their village doctors. Overall, half of the patients with hypertension achieved the BP control goal (BP<140/90 mm Hg).
Conclusions: Awareness and simple health messages increase provider visit, reduce blood pressure and improve BP control in hypertensive Bangladeshis. Longer-term follow-up is required to verify the sustainability.
Keywords: EPIDEMIOLOGY; PRIMARY CARE; PUBLIC HEALTH.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical