

Prevention of colonization and infection by Klebsiella pneumoniae carbapenemase-producing enterobacteriaceae in long-term acute-care hospitals
- PMID: 25537877
- PMCID: PMC8381216
- DOI: 10.1093/cid/ciu1173
Prevention of colonization and infection by Klebsiella pneumoniae carbapenemase-producing enterobacteriaceae in long-term acute-care hospitals
Abstract
Background: Klebsiella pneumoniae carbapenemase-producing Enterobacteriaceae (hereafter "KPC") are an increasing threat to healthcare institutions. Long-term acute-care hospitals (LTACHs) have especially high prevalence of KPC.
Methods: Using a stepped-wedge design, we tested whether a bundled intervention (screening patients for KPC rectal colonization upon admission and every other week; contact isolation and geographic separation of KPC-positive patients in ward cohorts or single rooms; bathing all patients daily with chlorhexidine gluconate; and healthcare-worker education and adherence monitoring) would reduce colonization and infection due to KPC in 4 LTACHs with high endemic KPC prevalence. The study was conducted between 1 February 2010 and 30 June 2013; 3894 patients were enrolled during the preintervention period (lasting from 16 to 29 months), and 2951 patients were enrolled during the intervention period (lasting from 12 to 19 months).
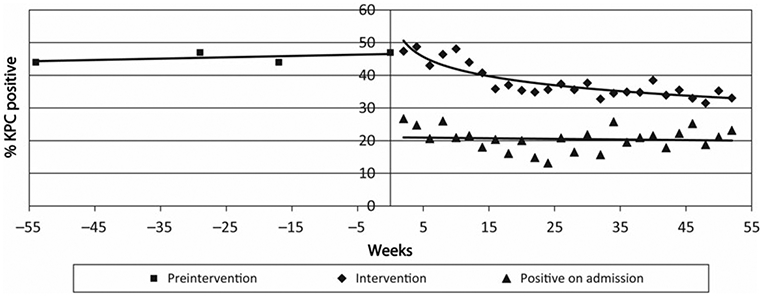
Results: KPC colonization prevalence was stable during preintervention (average, 45.8%; 95% confidence interval [CI], 42.1%-49.5%), declined early during intervention, then reached a plateau (34.3%; 95% CI, 32.4%-36.2%; P<.001 for exponential decline). During intervention, KPC admission prevalence remained high (average, 20.6%, 95% CI, 19.1%-22.3%). The incidence rate of KPC colonization fell during intervention, from 4 to 2 acquisitions per 100 patient-weeks (P=.004 for linear decline). Compared to preintervention, average rates of clinical outcomes declined during intervention: KPC in any clinical culture (3.7 to 2.5/1000 patient-days; P=.001), KPC bacteremia (0.9 to 0.4/1000 patient-days; P=.008), all-cause bacteremia (11.2 to 7.6/1000 patient-days; P=.006) and blood culture contamination (4.9 to 2.3/1000 patient-days; P=.03).
Conclusions: A bundled intervention was associated with clinically important and statistically significant reductions in KPC colonization, KPC infection, all-cause bacteremia, and blood culture contamination in a high-risk LTACH population.
Keywords: Klebsiella pneumoniae carbapenemase; carbapenem-resistant Enterobacteriaceae; healthcare-associated infection; infection prevention; long-term acute-care hospital.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures



References
-
- Maragakis LL, Perencevich EN, Cosgrove SE. Clinical and economic burden of antimicrobial resistance. Expert Rev Anti Infect Ther 2008; 6:751–63. - PubMed
-
- Nordmann P, Cornaglia G. Carbapenemase-producing Enterobacteriaceae: a call for action! Clin Microbiol Infect 2011; 18:411–2. - PubMed
-
- Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol 2008; 29:1099–106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
