

Critical care issues in solid organ injury: Review and experience in a tertiary trauma center
- PMID: 25538517
- PMCID: PMC4268524
- DOI: 10.4103/1658-354X.144065
Critical care issues in solid organ injury: Review and experience in a tertiary trauma center
Abstract
Background and aim: Solid organ (spleen and liver) injuries are dreaded by both surgeons and anesthesiologists because of associated high morbidity and mortality. The purpose of this review is to describe our experience of critical care concerns in solid organ injury, which otherwise has been poorly addressed in the literature.
Materials and methods: Retrospective cohort of solid organ injury (spleen and liver) patients was done from January 2010 to December 2011 in tertiary level trauma Center.
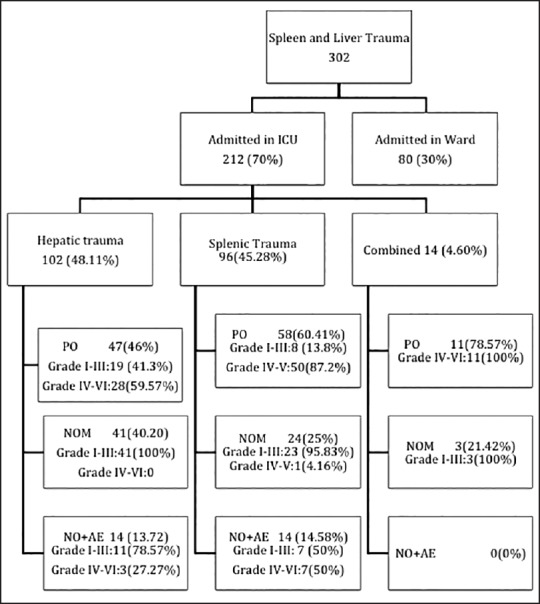
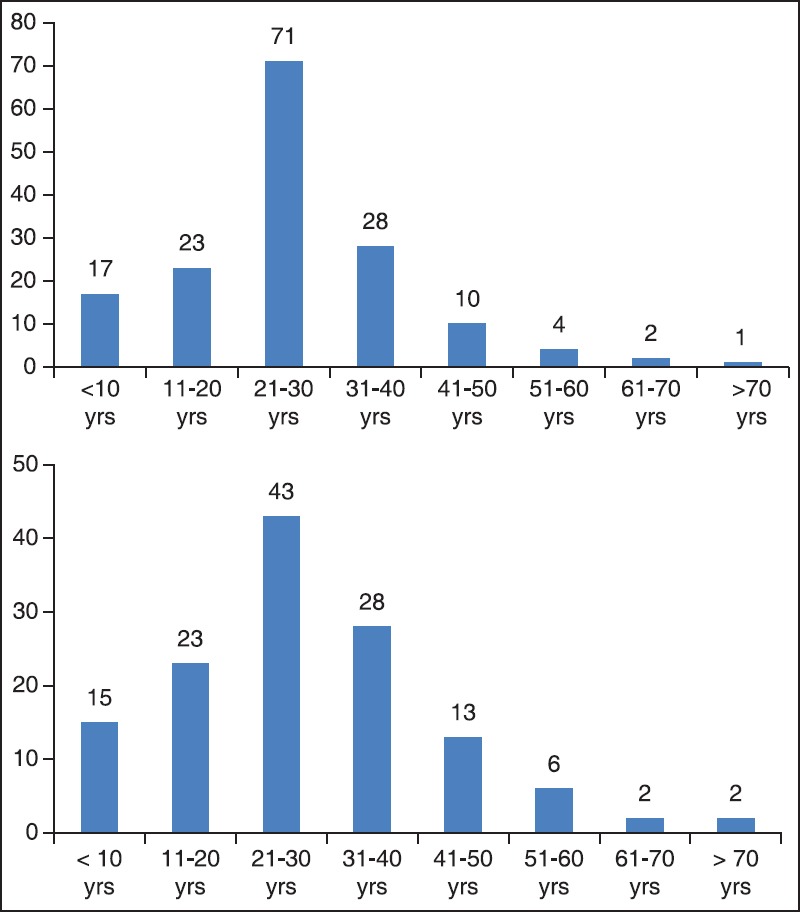
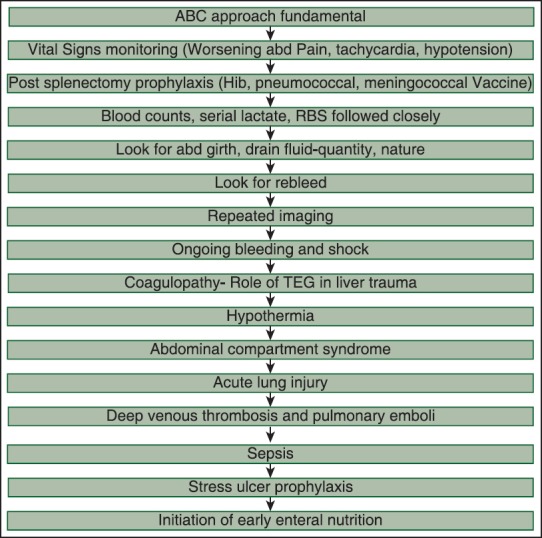
Results: Out of 624 abdominal trauma patients, a total of 212 patients (70%) were admitted in intensive care unit (ICU). Their ages ranged from 6 to 74 years (median 24 years). Nearly 89% patients in liver trauma and 84% patients in splenic trauma were male. Mechanism of injury was blunt abdominal trauma in 96% patients and the most common associated injury was chest trauma. Average injury severity score, sequential organ failure assessment, lactate on admission was 16.84, 4.34 and 3.42 mmol/L and that of dying patient were 29.70, 7.73 and 5.09 mmol/L, respectively. Overall mortality of ICU admitted solid organ injury was 15.55%. Major issues of concern in splenic injury were hemorrhagic shock, overwhelming post-splenectomy infection and post-splenectomy vaccination. Issues raised in liver injury are damage control surgery, deadly triad, thromboelastography guided transfusion protocols and hemostatic agents.
Conclusions: A protocol-based and multidisciplinary approach in high dependency unit can significantly reduce morbidity and mortality in patients with solid organ injury.
Keywords: Critical care; deadly triad; hepatic injury; liver trauma; solid organ injury; splenic trauma.
Conflict of interest statement
Figures
References
-
- Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. Organ injury scaling: Spleen and liver (1994 revision) J Trauma. 1995;38:323–4. - PubMed
-
- Notash AY, Amoli HA, Nikandish A, Kenari AY, Jahangiri F, Khashayar P. Non-operative management in blunt splenic trauma. Emerg Med J. 2008;25:210–2. - PubMed
-
- Malhotra AK, Latifi R, Fabian TC, Ivatury RR, Dhage S, Bee TK, et al. Multiplicity of solid organ injury: Influence on management and outcomes after blunt abdominal trauma. J Trauma. 2003;54:925–9. - PubMed
-
- Yanar H, Ertekin C, Taviloglu K, Kabay B, Bakkaloglu H, Guloglu R. Nonoperative treatment of multiple intra-abdominal solid organ injury after blunt abdominal trauma. J Trauma. 2008;64:943–8. - PubMed
-
- Eberle BM, Schnüriger B, Inaba K, Cestero R, Kobayashi L, Barmparas G, et al. Thromboembolic prophylaxis with low-molecular-weight heparin in patients with blunt solid abdominal organ injuries undergoing nonoperative management: Current practice and outcomes. J Trauma. 2011;70:141–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
