

What are the Best Animal Models for Testing Early Intervention in Cerebral Palsy?
- PMID: 25538677
- PMCID: PMC4255621
- DOI: 10.3389/fneur.2014.00258
What are the Best Animal Models for Testing Early Intervention in Cerebral Palsy?
Abstract
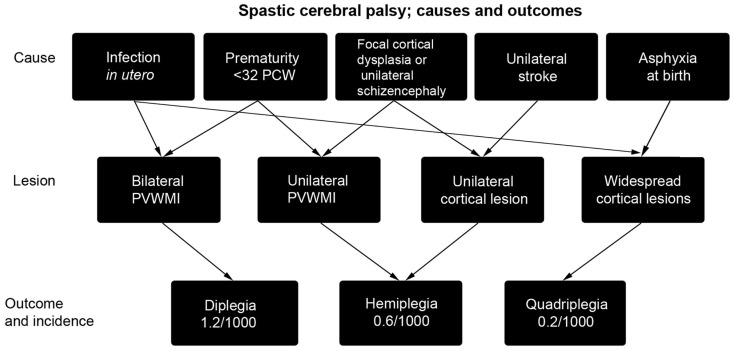
Interventions to treat cerebral palsy should be initiated as soon as possible in order to restore the nervous system to the correct developmental trajectory. One drawback to this approach is that interventions have to undergo exceptionally rigorous assessment for both safety and efficacy prior to use in infants. Part of this process should involve research using animals but how good are our animal models? Part of the problem is that cerebral palsy is an umbrella term that covers a number of conditions. There are also many causal pathways to cerebral palsy, such as periventricular white matter injury in premature babies, perinatal infarcts of the middle cerebral artery, or generalized anoxia at the time of birth, indeed multiple causes, including intra-uterine infection or a genetic predisposition to infarction, may need to interact to produce a clinically significant injury. In this review, we consider which animal models best reproduce certain aspects of the condition, and the extent to which the multifactorial nature of cerebral palsy has been modeled. The degree to which the corticospinal system of various animal models human corticospinal system function and development is also explored. Where attempts have already been made to test early intervention in animal models, the outcomes are evaluated in light of the suitability of the model.
Keywords: cerebral palsy; corticospinal tract; hypoxia/ischemia; perinatal stroke; periventricular white matter injury.
Figures



References
-
- Stanley F, Blair E, Alberman E. Cerebral Palsies: Epidemiology and Causal Pathways. Clinics in Developmental Medicine No. 151. London: Mac Keith Press; (2000).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources