

The economic burden of pulmonary arterial hypertension (PAH) in the US on payers and patients
- PMID: 25539602
- PMCID: PMC4301626
- DOI: 10.1186/s12913-014-0676-0
The economic burden of pulmonary arterial hypertension (PAH) in the US on payers and patients
Abstract
Background: Pulmonary arterial hypertension (PAH) is a rare condition that can ultimately lead to right heart failure and death. In this study we estimated the health care costs and resource utilization associated with PAH in a large US managed care health plan.
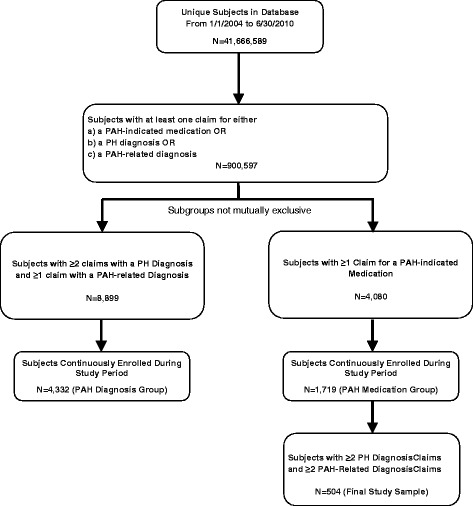
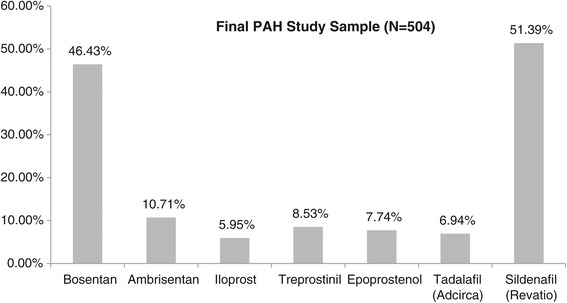
Methods: Subjects with claims-based evidence of PAH from 1/1/2004 to 6/30/2010 (identification period) were selected. To be included in the final PAH study sample, subjects were required to have ≥2 claims with a primary PH diagnosis; ≥2 claims with a PAH related-diagnosis (connective tissue diseases, congenital heart diseases, portal hypertension); and ≥1 claim with evidence of a PAH-indicated medication. The earliest date of a claim with evidence of PAH-indicated medication during the identification period was set as the index date. Health care costs and resource utilization were compared between an annualized baseline period and a 12 month follow-up period.
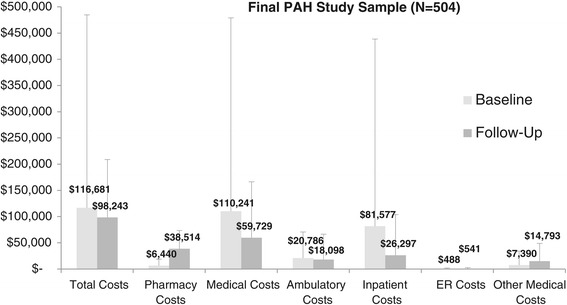
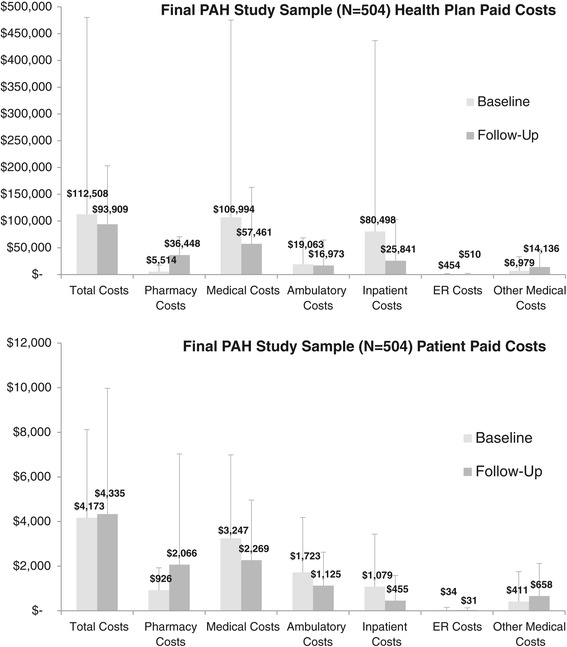
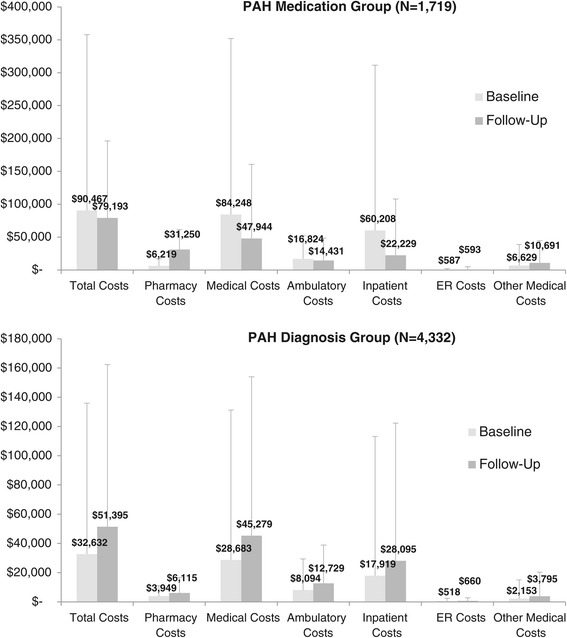
Results: 504 PAH subjects were selected for the final study cohort. Estimated average total health care costs were approximately 16% lower in the follow-up period compared to the baseline period (follow-up costs = $98,243 [SD = 110,615] vs. baseline costs = $116,681 [SD = 368,094], p < 0.001), but substantively high in each period relative to costs reported for other chronic diseases. Pharmacy costs were significantly higher in the follow-up period vs. the baseline period, ($38,514 [SD = 34,817] vs. $6,440 [SD = 12,186], p < 0.001) but medical costs were significantly lower in the follow-up vs. baseline ($59,729 [SD = 106,683] vs. $110,241 [SD = 368,725], p < 0.001). These costs were mirrored in health-care resource utilization estimates. The average counts of ambulatory visits and inpatient stays were lower in the follow-up vs. the baseline (both p < 0.001). Results varied in exploratory analyses when less restrictive subject identification algorithms were used.
Conclusions: Subjects with evidence of PAH had substantively high health care costs. Medical costs appeared to decrease following PAH medication use, but with a concomitant increase in pharmacy costs.
Figures
References
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G, ESC Committee for Practice Guidelines (CPG) Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT) Eur Heart J. 2009;30:2493–2537. doi: 10.1093/eurheartj/ehp297. - DOI - PubMed
-
- Machado RD, Pauciulo MW, Thomson JR, Lane KB, Morgan NV, Wheeler L, Phillips JA, 3rd, Newman J, Williams D, Galiè N, Manes A, McNeil K, Yacoub M, Mikhail G, Rogers P, Corris P, Humbert M, Donnai D, Martensson G, Tranebjaerg L, Loyd JE, Trembath RC, Nichols WC. BMPR2 haploinsufficiency as the inherited molecular mechanism for primary pulmonary hypertension. Am J Hum Genet. 2001;68:92–102. doi: 10.1086/316947. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
