

Limb function and quality of life after various reconstruction methods according to tumor location following resection of osteosarcoma in distal femur
- PMID: 25539904
- PMCID: PMC4364625
- DOI: 10.1186/1471-2474-15-453
Limb function and quality of life after various reconstruction methods according to tumor location following resection of osteosarcoma in distal femur
Abstract
Background: We tried to compare the functional and psychosocial outcomes after various reconstruction methods according to tumor location following resection of osteosarcoma in distal femur.
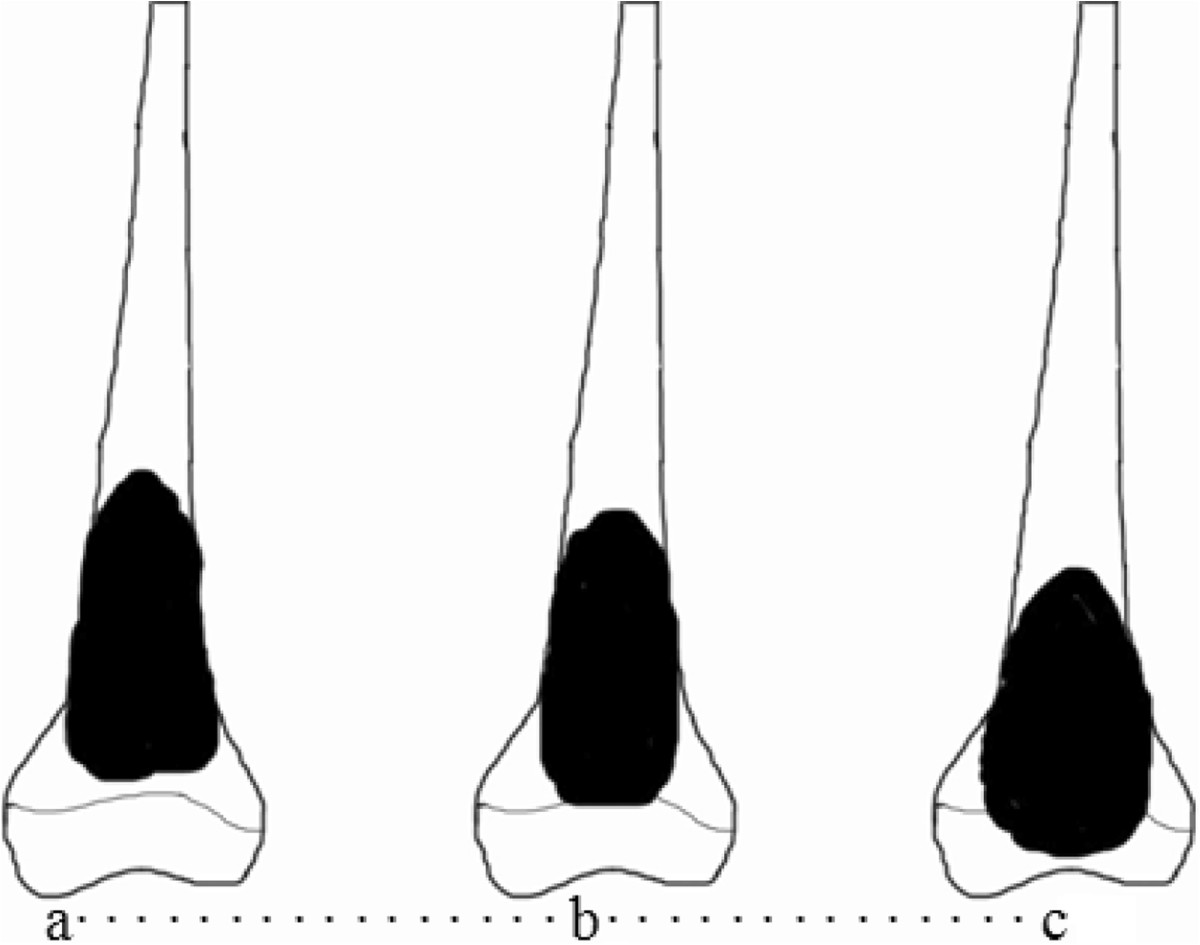
Methods: We retrospectively reviewed 51 patients who underwent limb-salvage surgery of osteosarcoma in distal femur in our institution, 30 males and 21 females with an average age of 21 years (range 13-51 years). We classified osteosarcoma in distal femur into 3 types, and organized affected limb reconstruction methods after wide resection. MSTS and QOL scores were used to analyze the functional and psychological outcomes.
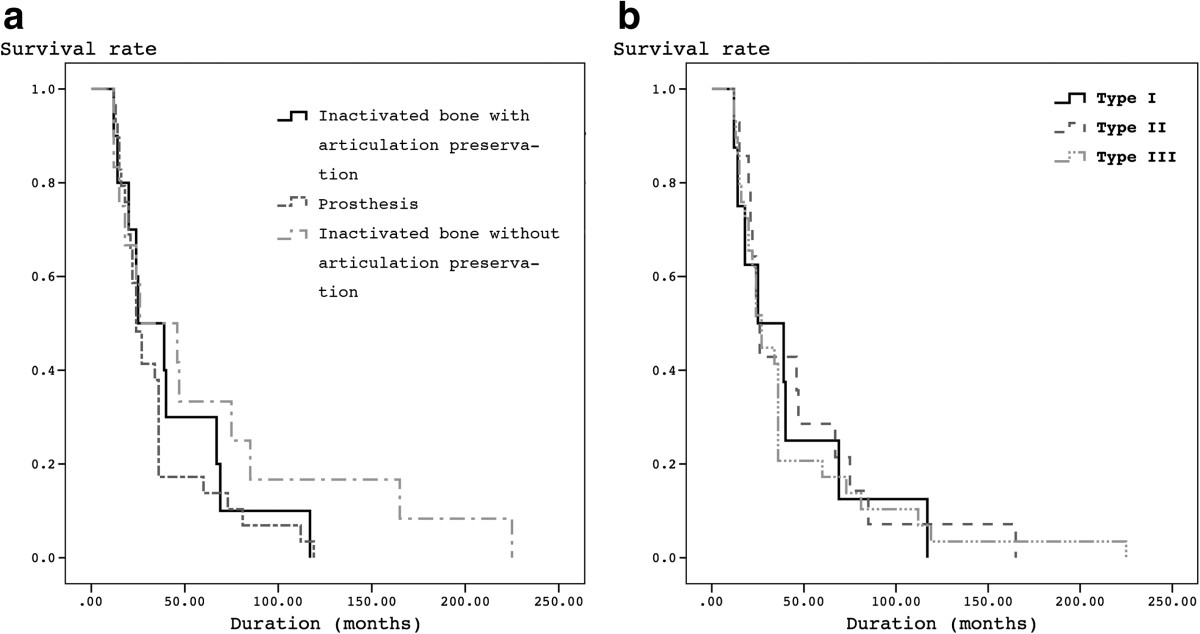
Results: After a mean follow-up of 43 months (12-225 months), there is no difference on functional results and QOL scores among three reconstruction groups (p > 0.05) and among three types groups (p > 0.05). No difference could be noticed on tumor-free survival and total survival among three reconstruction groups (p > 0.05) and three type groups (p > 0.05). In ≤2-year, better functional scores could be found in prosthesis group, rather than the other two inactivated-bone groups (p < 0.05).
Conclusions: Biological reconstruction with alcohol-inactivated autograft replantation could avoid prosthesis related complications and achieved comparable results with prosthesis following resection of osteosarcoma in distal femur. Different reconstruction options could be chosen according to tumor location, such as the distance to Insall line.
Figures


Similar articles
-
Impacts of Tumor Location, Nature and Bone Destruction of Extremity Osteosarcoma on Selection of Limb Salvage Operative Procedure.Orthop Surg. 2016 May;8(2):139-49. doi: 10.1111/os.12237. Orthop Surg. 2016. PMID: 27384722 Free PMC article.
-
Functional outcome of surgical treatment of adults with extremity osteosarcoma after megaprosthetic reconstruction-single-center experience.J Orthop Surg Res. 2019 Nov 7;14(1):346. doi: 10.1186/s13018-019-1379-3. J Orthop Surg Res. 2019. PMID: 31699134 Free PMC article.
-
Reconstruction with Custom Unicondylar Hemiarthroplasty following Tumor Resection: A Case Series and Review of the Literature.J Knee Surg. 2020 Aug;33(8):818-824. doi: 10.1055/s-0039-1688556. Epub 2019 May 8. J Knee Surg. 2020. PMID: 31067588 Review.
-
[Epiphysis preserving by physeal distraction for treatment of femur osteosarcoma in children].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 Apr;27(4):423-7. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 23757868 Chinese.
-
Outcomes of Expandable Prostheses for Primary Bone Malignancies in Skeletally Immature Patients: A Systematic Review and Pooled Data Analysis.J Pediatr Orthop. 2020 Jul;40(6):e487-e497. doi: 10.1097/BPO.0000000000001459. J Pediatr Orthop. 2020. PMID: 32501921
Cited by
-
Limb-salvage treatment of en-block resected distal femoral tumors with endoprosthesis of all-polyethylene tibial component: a 9-year follow-up study.Onco Targets Ther. 2016 Sep 13;9:5361-5369. doi: 10.2147/OTT.S106608. eCollection 2016. Onco Targets Ther. 2016. PMID: 27695342 Free PMC article.
-
All-polyethylene tibial components in distal femur limb-salvage surgery: a finite element analysis based on promising clinical outcomes.J Orthop Surg Res. 2017 Apr 4;12(1):57. doi: 10.1186/s13018-017-0555-6. J Orthop Surg Res. 2017. PMID: 28376828 Free PMC article.
-
Impacts of Tumor Location, Nature and Bone Destruction of Extremity Osteosarcoma on Selection of Limb Salvage Operative Procedure.Orthop Surg. 2016 May;8(2):139-49. doi: 10.1111/os.12237. Orthop Surg. 2016. PMID: 27384722 Free PMC article.
-
The application of 3D printed surgical guides in resection and reconstruction of malignant bone tumor.Oncol Lett. 2017 Oct;14(4):4581-4584. doi: 10.3892/ol.2017.6749. Epub 2017 Aug 11. Oncol Lett. 2017. PMID: 29085456 Free PMC article.
-
The therapeutic effects of X-ray devitalization and replantation and alcoholic devitalization and replantation in adolescent patients with lower limb osteosarcoma.Am J Transl Res. 2021 May 15;13(5):5547-5553. eCollection 2021. Am J Transl Res. 2021. PMID: 34150156 Free PMC article.
References
-
- Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980;2003:4–18. - PubMed
-
- Yu XC, Liu XP, Zhou Y, Fu ZH, Song RX, Sun HN, Xu M. Inactivated bone replantation with preservation of the epiphysis for osteosarcoma in children. Orthop J China. 2007;15:811–813.
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/15/453/prepub
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
