

Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit
- PMID: 25540068
- PMCID: PMC4533730
- DOI: 10.1093/bja/aeu442
Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit
Abstract
Background: Emergence from anaesthesia is often accompanied by signs of delirium, including fluctuating mental status and inattention. The evolution of these signs of delirium requires investigation since delirium in the post-anaesthesia care unit (PACU) may be associated with worse outcomes.
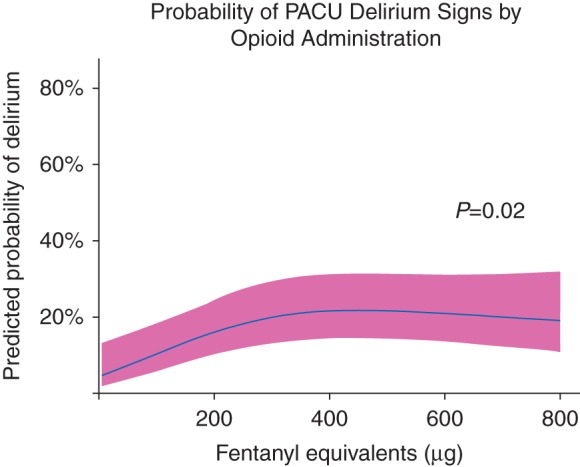
Methods: Adult patients emerging from anaesthesia were assessed for agitated emergence in the operating room using the Richmond Agitation-Sedation Scale (RASS). The Confusion Assessment Method for the Intensive Care Unit was then used to evaluate delirium signs at PACU admission and during PACU stay at 30 min, 1 h, and discharge. Signs consistent with delirium were classified as hyperactive vs hypoactive based upon a positive CAM-ICU assessment and the concomitant RASS score. Multivariable logistic regression was utilized to assess potential risk factors for delirium during PACU stay including age, American Society of Anesthesiologists classification, and opioid and benzodiazepine exposure.
Results: Among 400 patients enrolled, 19% had agitated emergence. Delirium signs were present at PACU admission, 30 min, 1 h, and PACU discharge in 124 (31%), 59 (15%), 32 (8%), and 15 (4%) patients, respectively. In patients with delirium signs, hypoactive signs were present in 56% at PACU admission and in 92% during PACU stay. Perioperative opioids were associated with delirium signs during PACU stay (P=0.02).
Conclusions: A significant proportion of patients develop delirium signs in the immediate postoperative period, primarily manifesting with a hypoactive subtype. These signs often persist to PACU discharge, suggesting the need for structured delirium monitoring in the PACU to identify patients potentially at risk for worse outcomes in the postoperative period.
Keywords: anaesthesia; complications; delirium.
© The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA 2001; 286: 2703–10 - PubMed
-
- Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med 2007; 33: 66–73 - PubMed
-
- Franco K, Litaker D, Locala J, Bronson D. The cost of delirium in the surgical patient. Psychosomatics 2001; 42: 68–73 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
