

Risk of distal embolization with stent retriever thrombectomy and ADAPT
- PMID: 25540180
- PMCID: PMC4752657
- DOI: 10.1136/neurintsurg-2014-011491
Risk of distal embolization with stent retriever thrombectomy and ADAPT
Abstract
Background: There is a discrepancy in clinical outcomes and the achieved recanalization rates with stent retrievers in the endovascular treatment of ischemic stroke. It is our hypothesis that procedural release of embolic particulate may be one contributor to poor outcomes and is a modifiable risk. The goal of this study is to assess various treatment strategies that reduce the risk of distal emboli.
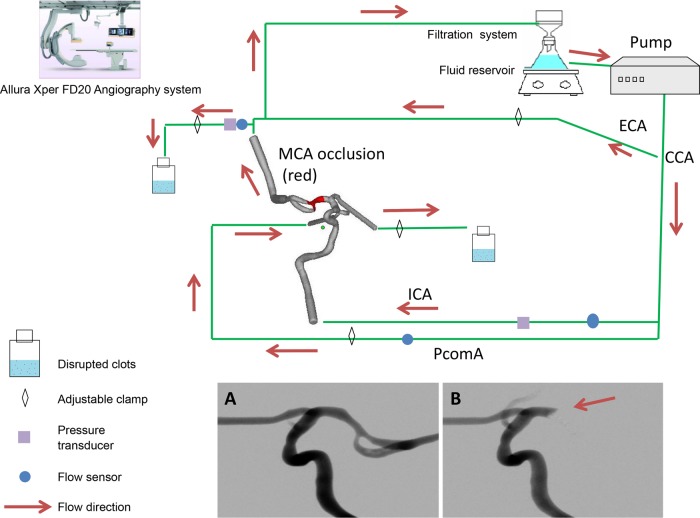
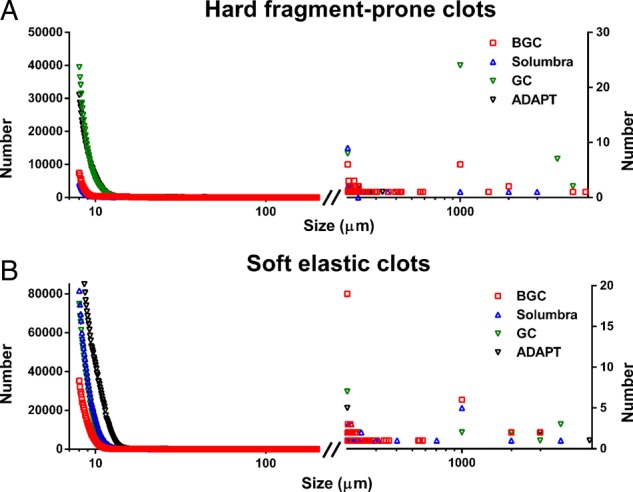
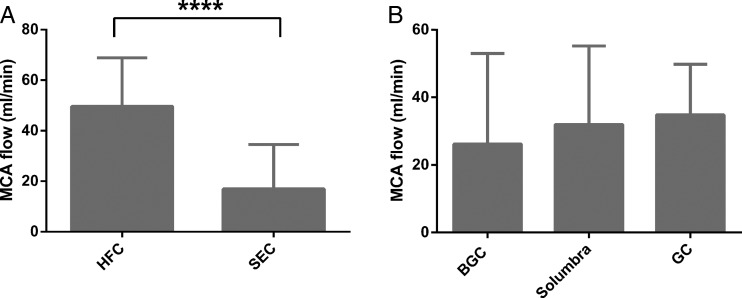
Methods: Mechanical thrombectomy was simulated in a vascular phantom with collateral circulation. Hard fragment-prone clots (HFC) and soft elastic clots (SECs) were used to generate middle cerebral artery (MCA) occlusions that were retrieved by the Solitaire FR devices through (1) an 8 Fr balloon guide catheter (BGC), (2) a 5 Fr distal access catheter at the proximal aspect of the clot in the MCA (Solumbra), or (3) a 6 Fr guide catheter with the tip at the cervical internal carotid artery (guide catheter, GC). Results from mechanical thrombectomy were compared with those from direct aspiration using the Penumbra 5MAX catheter. The primary endpoint was the size distribution of emboli to the distribution of the middle and anterior cerebral arteries.
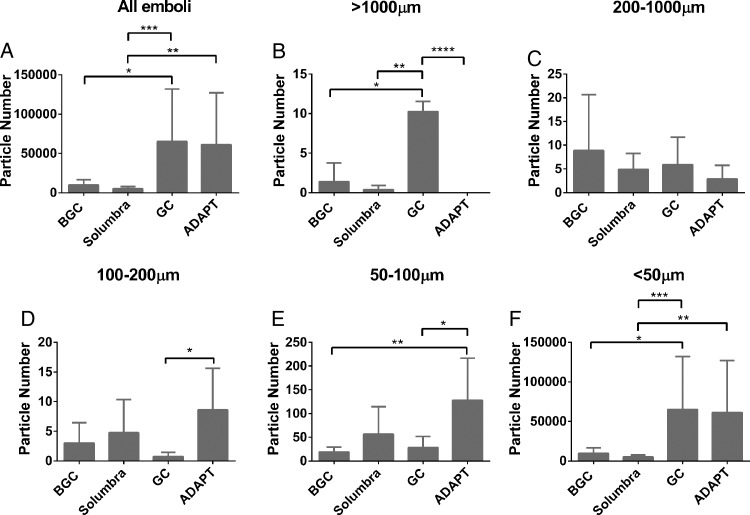
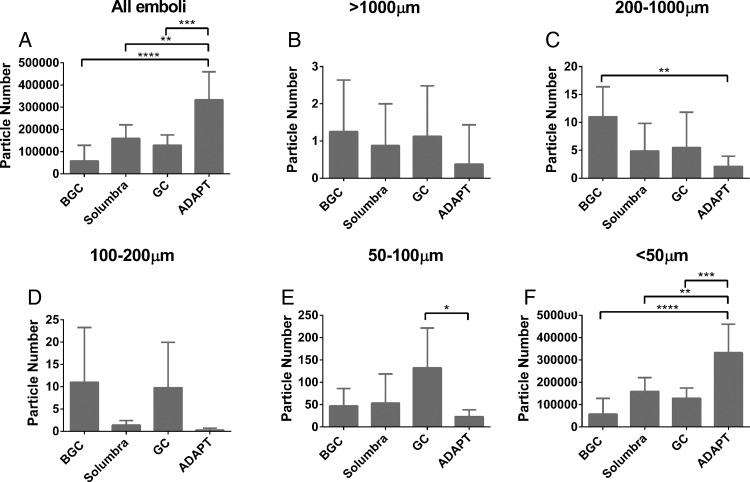
Results: Solumbra was the most efficient method for reducing HFC fragments (p<0.05) while BGC was the best method for preventing SEC fragmentation (p<0.05). The risk of forming HFC distal emboli (>1000 µm) was significantly increased using GC. A non-statistically significant benefit of direct aspiration was observed in several subgroups of emboli with size 50-1000 µm. However, compared with the stent-retriever mechanical thrombectomy techniques, direct aspiration significantly increased the risk of SEC fragmentation (<50 µm) by at least twofold.
Conclusions: The risk of distal embolization is affected by the catheterization technique and clot mechanics.
Keywords: Device; Intervention; Stroke; Thrombectomy.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures

References
-
- Nguyen TN, Malisch T, Castonguay A, et al. Balloon guide catheter improves recanalisation, procedure time, and clinical outcomes with Solitaire in acute stroke: analysis of the NASA Registry. J Neurointerv Surg 2013;5:A2–3. 10.1136/neurintsurg-2013-010870.4 - DOI
-
- Humphries W, Hoit D, Doss VT, et al. Distal aspiration with retrievable stent assisted thrombectomy for the treatment of acute ischemic stroke. J Neurointerv Surg 2015;7:90–4.. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous