

Small nerve fiber involvement in CMT1A
- PMID: 25540311
- PMCID: PMC4336000
- DOI: 10.1212/WNL.0000000000001188
Small nerve fiber involvement in CMT1A
Abstract
Objective: To assess the involvement of small nerve fibers in Charcot-Marie-Tooth type 1A (CMT1A).
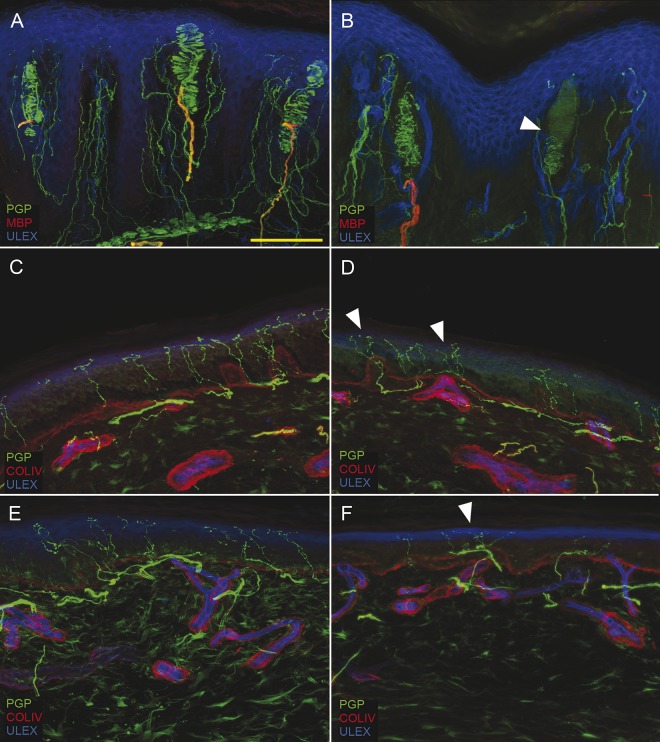
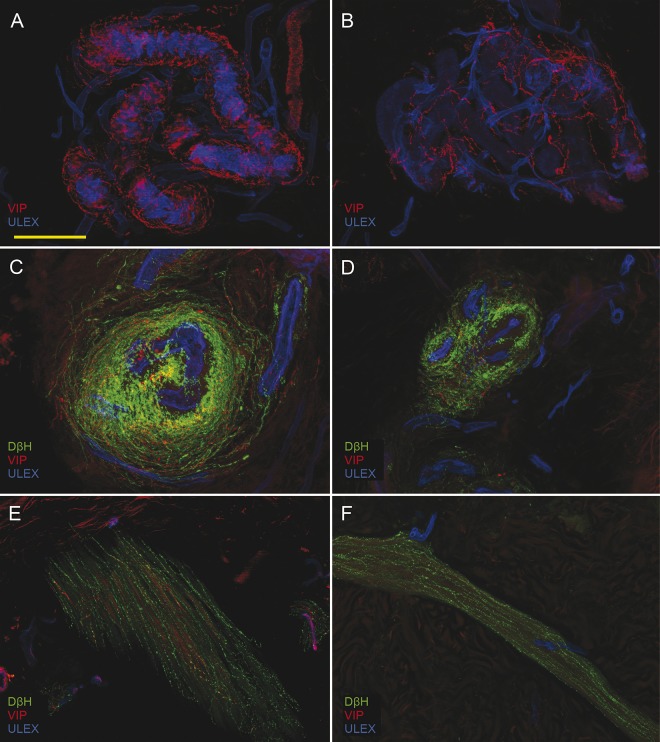
Methods: We used indirect immunofluorescence and confocal microscopy on punch biopsies from glabrous (fingertip) and hairy (thigh and leg) skin of 20 unrelated patients with CMT1A to quantify somatic and autonomic nerve fibers. In particular, we quantified epidermal nerve fibers (ENF), Meissner corpuscles (MC), intrapapillary myelinated endings (IME), and sudomotor nerves. We correlated morphologic data with findings from quantitative sensory testing, sudomotor output, sympathetic skin response, and cardiovascular reflexes. A control population of healthy age- and sex-matched controls was included with a matching ratio of 1:2.
Results: We found a length-dependent loss of ENFs that worsened with aging. We also observed a loss of MCs, IMEs, and sudomotor nerves. The loss of ENF at distal leg correlated with the increase in heat-pain thresholds (p < 0.05) and with tactile thresholds (p < 0.05). Sudomotor nerve fiber loss correlated with ENF density (p < 0.05) and sweating output (p < 0.001).
Conclusions: We demonstrated through morphologic, physical, and psychophysical testing that small somatic and autonomic fibers are abnormal and cause symptoms in patients with CMT1A. Awareness of such symptoms by the clinician could lead to better treatment.
© 2014 American Academy of Neurology.
Figures
References
-
- Skre H. Genetic and clinical aspects of Charcot-Marie-Tooth's disease. Clin Genet 1974;6:98–118. - PubMed
-
- Shy M, Lupski JR, Chance PF, Klein CJ, Dyck P. The hereditary motor and sensory neuropathies: an overview of the clinical, genetic, electrophysiologic and pathologic features. In: Dyck PJ, Thomas PK, eds. Peripheral Neuropathy, 4th ed Philadelphia: WB Saunders; 2005:1623–1658.
-
- Colomban C, Micallef J, Lefebvre MN, et al. Clinical spectrum and gender differences in a large cohort of Charcot-Marie-Tooth type 1A patients. J Neurol Sci 2014;336:155–160. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical