

Combining functional and tubular damage biomarkers improves diagnostic precision for acute kidney injury after cardiac surgery
- PMID: 25541128
- PMCID: PMC4310455
- DOI: 10.1016/j.jacc.2014.09.066
Combining functional and tubular damage biomarkers improves diagnostic precision for acute kidney injury after cardiac surgery
Erratum in
- J Am Coll Cardiol. 2015 Mar 24;65(11):1158-9
Abstract
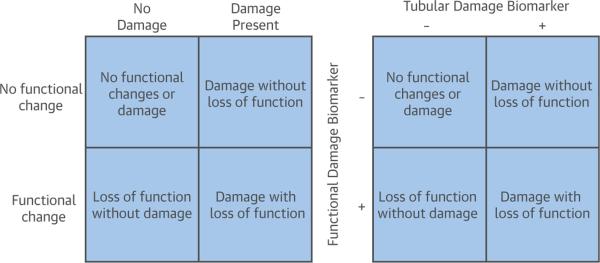
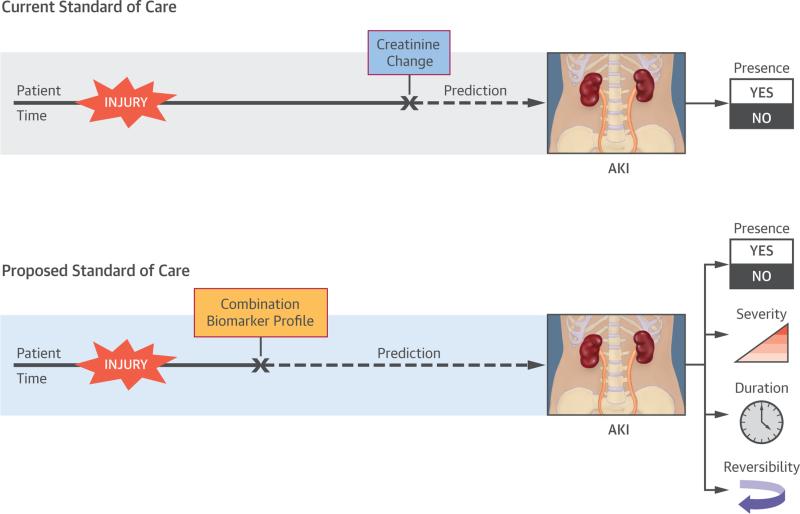
Background: Increases in serum creatinine (ΔSCr) from baseline signify acute kidney injury (AKI) but offer little granular information regarding its characteristics. The 10th Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) suggested that combining AKI biomarkers would provide better precision for AKI course prognostication.
Objectives: This study investigated the value of combining a functional damage biomarker (plasma cystatin C [pCysC]) with a tubular damage biomarker (urine neutrophil gelatinase-associated lipocalin [uNGAL]), forming a composite biomarker for prediction of discrete characteristics of AKI.
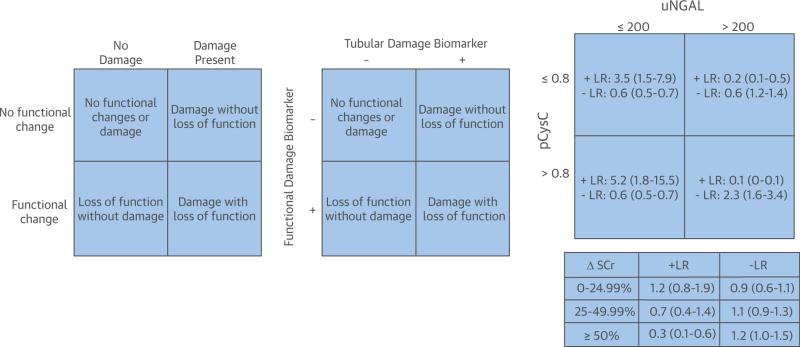
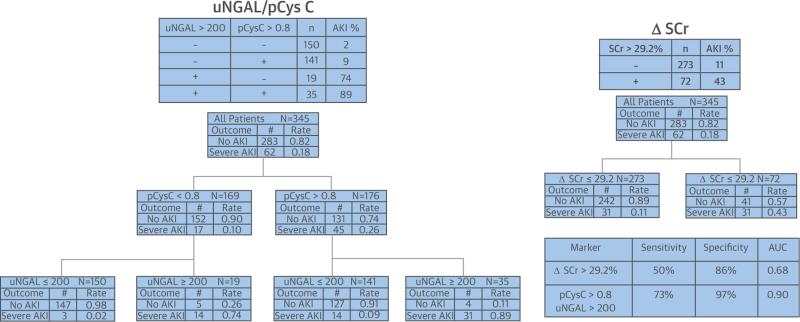
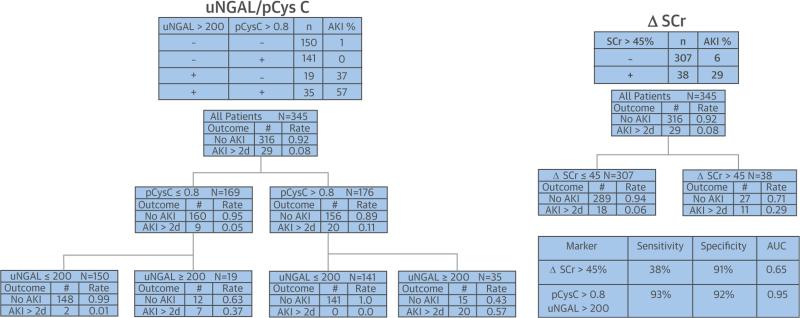
Methods: Data from 345 children after cardiopulmonary bypass (CPB) were analyzed. Severe AKI was defined as Kidney Disease Global Outcomes Initiative stages 2 to 3 (≥100% ΔSCr) within 7 days of CPB. Persistent AKI lasted >2 days. SCr in reversible AKI returned to baseline ≤48 h after CPB. The composite of uNGAL (>200 ng/mg urine Cr = positive [+]) and pCysC (>0.8 mg/l = positive [+]), uNGAL+/pCysC+, measured 2 h after CPB initiation, was compared to ΔSCr increases of ≥50% for correlation with AKI characteristics by using predictive probabilities, likelihood ratios (LR), and area under the curve receiver operating curve (AUC-ROC) values [Corrected].
Results: Severe AKI occurred in 18% of patients. The composite uNGAL+/pCysC+ demonstrated a greater likelihood than ΔSCr for severe AKI (+LR: 34.2 [13.0:94.0] vs. 3.8 [1.9:7.2]) and persistent AKI (+LR: 15.6 [8.8:27.5] versus 4.5 [2.3:8.8]). In AKI patients, the uNGAL-/pCysC+ composite was superior to ΔSCr for prediction of transient AKI. Biomarker composites carried greater probability for specific outcomes than ΔSCr strata.
Conclusions: Composites of functional and tubular damage biomarkers are superior to ΔSCr for predicting discrete characteristics of AKI.
Keywords: Acute Dialysis Quality Initiative; acute kidney injury phenotypes; biomarker combinations; cardiac surgery; functional acute kidney injury; pediatric acute kidney injury.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Improving detection of cardiac surgery-associated acute kidney injury.J Am Coll Cardiol. 2014 Dec 30;64(25):2763-4. doi: 10.1016/j.jacc.2014.09.065. J Am Coll Cardiol. 2014. PMID: 25541129 No abstract available.
References
-
- Lameire NH, Bagga A, Cruz D, et al. Acute kidney injury: an increasing global concern. Lancet. 2013;382:170–9. - PubMed
-
- Rewa O, Bagshaw SM. Acute kidney injury—epidemiology, outcomes and economics. Nat Rev Nephrol. 2014;10:193–207. - PubMed
-
- Hoste EA, Kellum JA, Katz NM, et al. Epidemiology of acute kidney injury. Contrib Nephrol. 2010;165:1–8. - PubMed
-
- Fortenberry JD, Paden ML, Goldstein SL. Acute kidney injury in children: an update on diagnosis and treatment. Pediatr Clin North Am. 2013;60:669–88. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group Clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
