

Uterine artery embolization for symptomatic uterine fibroids
- PMID: 25541260
- PMCID: PMC11285296
- DOI: 10.1002/14651858.CD005073.pub4
Uterine artery embolization for symptomatic uterine fibroids
Abstract
Background: Uterine fibroids cause heavy prolonged bleeding, pain, pressure symptoms and subfertility. The traditional method of treatment has been surgery as medical therapies have not proven effective. Uterine artery embolization has been reported to be an effective and safe alternative to treat fibroids in women not desiring future fertility. There is a significant body of evidence that is based on case controlled studies and case reports. This is an update of the review previously published in 2012.
Objectives: To review the benefits and risks of uterine artery embolization (UAE) versus other medical or surgical interventions for symptomatic uterine fibroids.
Search methods: We searched sources including the Cochrane Menstrual Disorders and Subfertility Group Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE and trial registries. The search was last conducted in April 2014. We contacted authors of eligible randomised controlled trials to request unpublished data.
Selection criteria: Randomised controlled trials (RCTs) of UAE versus any medical or surgical therapy for symptomatic uterine fibroids. The primary outcomes of the review were patient satisfaction and live birth rate (among women seeking live birth).
Data collection and analysis: Two of the authors (AS and JKG) independently selected studies, assessed quality and extracted data. Evidence quality was assessed using GRADE methods.
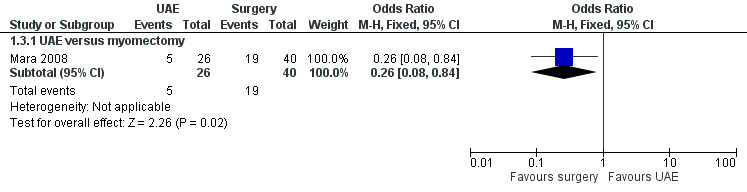
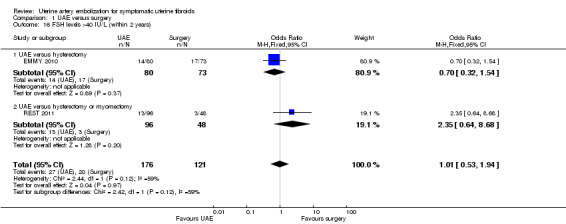
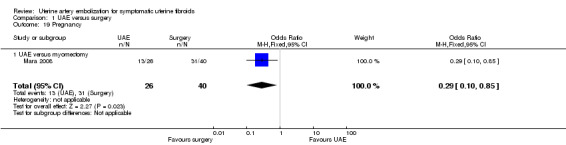
Main results: Seven RCTs with 793 women were included in this review. Three trials compared UAE with abdominal hysterectomy, two trials compared UAE with myomectomy, and two trials compared UAE with either type of surgery (53 hysterectomies and 62 myomectomies).With regard to patient satisfaction rates, our findings were consistent with satisfaction rates being up to 41% lower or up to 48% higher with UAE compared to surgery within 24 months of having the procedure (odds ratio (OR) 0.94; 95% confidence interval (CI) 0.59 to 1.48, 6 trials, 640 women, I(2) = 5%, moderate quality evidence). Findings were also inconclusive at five years of follow-up (OR 0.90; 95% CI 0.45 to 1.80, 2 trials, 295 women, I(2) = 0%, moderate quality evidence). There was some indication that UAE may be associated with less favourable fertility outcomes than myomectomy, but it was very low quality evidence from a subgroup of a single study and should be regarded with extreme caution (live birth: OR 0.26; 95% CI 0.08 to 0.84; pregnancy: OR 0.29; 95% CI 0.10 to 0.85, 1 study, 66 women).Similarly, for several safety outcomes our findings showed evidence of a substantially higher risk of adverse events in either arm or of no difference between the groups. This applied to intra-procedural complications (OR 0.91; 95% CI 0.42 to 1.97, 4 trials, 452 women, I(2) = 40%, low quality evidence), major complications within one year (OR 0.65; 95% CI 0.33 to 1.26, 5 trials, 611 women, I(2) = 4%, moderate quality evidence) and major complications within five years (OR 0.56; CI 0.27 to 1.18, 2 trials, 268 women). However, the rate of minor complications within one year was higher in the UAE group (OR 1.99; CI 1.41 to 2.81, 6 trials, 735 women, I(2) = 0%, moderate quality evidence) and two trials found a higher minor complication rate in the UAE group at up to five years (OR 2.93; CI 1.73 to 4.93, 2 trials, 268 women).UAE was associated with a higher rate of further surgical interventions (re-interventions within 2 years: OR 3.72; 95% CI 2.28 to 6.04, 6 trials, 732 women, I(2) = 45%, moderate quality evidence; within 5 years: OR 5.79; 95% CI 2.65 to 12.65, 2 trials, 289 women, I(2) = 65%). If we assumed that 7% of women will require further surgery within two years of hysterectomy or myomectomy, between 15% and 32% will require further surgery within two years of UAE.The evidence suggested that women in the UAE group were less likely to require a blood transfusion than women receiving surgery (OR 0.07; 95% CI 0.01 to 0.52, 2 trials, 277 women, I(2) = 0%). UAE was also associated with a shorter procedural time (two studies), shorter length of hospital stay (seven studies) and faster resumption of usual activities (six studies) in all studies that measured these outcomes; however, most of these data could not be pooled due to heterogeneity between the studies.The quality of the evidence varied, and was very low for live birth, moderate for satisfaction ratings, and moderate for most safety outcomes. The main limitations in the evidence were serious imprecision due to wide confidence intervals, failure to clearly report methods, and lack of blinding for subjective outcomes.
Authors' conclusions: When we compared patient satisfaction rates at up to two years following UAE versus surgery (myomectomy or hysterectomy) our findings are that there is no evidence of a difference between the interventions. Findings at five year follow-up were similarly inconclusive. There was very low quality evidence to suggest that myomectomy may be associated with better fertility outcomes than UAE, but this information was only available from a selected subgroup in one small trial.We found no clear evidence of a difference between UAE and surgery in the risk of major complications, but UAE was associated with a higher rate of minor complications and an increased likelihood of requiring surgical intervention within two to five years of the initial procedure. If we assume that 7% of women will require further surgery within two years of hysterectomy or myomectomy, between 15% and 32% will require further surgery within two years of UAE. This increase in the surgical re-intervention rate may balance out any initial cost advantage of UAE. Thus although UAE is a safe, minimally invasive alternative to surgery, patient selection and counselling are paramount due to the much higher risk of requiring further surgical intervention.
Conflict of interest statement
Mary Ann Lumsden took part in the REST clinical trial.
Figures
























Update of
-
Uterine artery embolization for symptomatic uterine fibroids.Cochrane Database Syst Rev. 2012 May 16;(5):CD005073. doi: 10.1002/14651858.CD005073.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Dec 26;(12):CD005073. doi: 10.1002/14651858.CD005073.pub4. PMID: 22592701 Updated.
References
References to studies included in this review
EMMY 2010 {published data only}
-
- Hehenkamp WJK, Volkers NA, Birnie E, Reekers JA, Ankum WM. Pain and return to daily activities after uterine artery embolization and hysterectomy in the treatment of symptomatic uterine fibroids: Results from the randomized EMMY trial. Cardiovascular Interventional Radiology 2006;29:179‐87. - PubMed
-
- Hehenkamp WJK, Volkers NA, Birnie E, Reekers JA, Ankum WM. Symptomatic uterine fibroids: Treatment with uterine artery embolization or hysterectomy ‐ results from the randomized clinical embolization versus hysterectomy (EMMY) trial. Radiology 2008;246(3):823‐32. - PubMed
-
- Hehenkamp WJK, Volkers NA, Broekmans FJM, Jong FH, Themmen APN, Birnie E, et al. Loss of ovarian reserve after uterine artery embolization: a randomised comparison with hysterectomy. Human Reproduction 2007;22:1996‐2005. - PubMed
-
- Hehenkamp WJK, Volkers NA, Donderwinkel PFJ, Blok S, Birnie E, Ankum WA, et al. Uterine artery embolization versus hysterectomy in the treatment of symptomatic uterine fibroids (EMMY trial): Peri‐ and postprocedural results from a randomized controlled trial. American Journal of Obstetrics and Gynecology 2005;193:1618‐29. - PubMed
-
- Volkers NA, Hehenkamp WJ, Smit P, Ankum WM, Reekers JA, Birnie E. Economic evaluation of uterine artery embolization versus hysterectomy in the treatment of symptomatic uterine fibroids: results from the randomized EMMY trial. Journal of Vascular Interventional Radiology 2008;19:1007‐17. - PubMed
FUME 2012 {published data only}
-
- Manyonda IT, Bratby M, Horst JS, Banu N, Gorti M, Belli A‐M. Uterine artery embolization versus myomectomy: Impact on quality of life ‐ results of the FUME (Fibroids of the Uterus: Myomectomy versus Embolization) trial. Cardiovascular and Interventional Radiology 2012;35(3):530‐6. - PubMed
Jun 2012 {published data only}
-
- Jun F, Yamin L, Xinli X, Zhe L, Min Z, Bo Z, Wenli G. Uterine artery embolization versus surgery for symptomatic uterine fibroids: a randomized controlled trial and a meta‐analysis of the literature. Archives of Gynecology and Obstetrics 2012;285:1407‐13. - PubMed
Mara 2008 {published data only}
-
- Mara M, Fucikovaa Z, Maskova J, Kuzela J, Haakova L. Uterine fibroid embolization versus myomectomy in women wishing to preserve fertility: preliminary results of a randomized controlled trial. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2006;126:226‐33. - PubMed
Pinto 2003 {published data only}
-
- Pinto I, Chimeno P, Romo L, Haya J, Cal M, Bajo J. Uterine fibroids: Uterine artery embolization versus abdominal hysterectomy for treatment. A prospective randomized and controlled trial. Radiology 2003;226(2):425‐31. - PubMed
REST 2011 {published data only}
-
- Edwards RD, Moss JG, Lumsden MA, Wu O, Murray LS, Twaddle S, et al. Uterine artery embolization versus surgery for symptomatic uterine fibroids. New England Journal of Medicine 2007;356:360‐70. - PubMed
-
- Moss JG, Cooper KG, Khaund A, Murray LS, Murray GD, Wu O, et al. Randomised comparison of uterine artery embolisation (UAE) with surgical treatment in patients with symptomatic uterine fibroids (REST trial): 5 year results. British Journal of Obstetrics and Gynaecology 2011;118(8):936‐44. - PubMed
-
- Rashid S, Khaund A, Murray LS, Moss JG, Cooper K, Lyons D, et al. The effects of uterine artery embolisation and surgical treatment on ovarian function in women with uterine fibroids. British Journal of Obstetrics and Gynaecology 2010;117:985‐9. - PubMed
Ruuskanen 2010 {published data only}
-
- Ruuskanen A, Hippelainen M, Sipola P, Manninen H. Uterine artery embolisation versus hysterectomy for leiomyomas: primary and 2‐year follow‐up results of a randomised prospective clinical trial. European Radiology 2010;20(10):2524‐32. - PubMed
References to studies excluded from this review
Hald 2007 {published data only}
-
- Hald K, Kløw NE, Qvigstad E, Istre O. Laparoscopic occlusion compared with embolization of uterine vessels: a randomized controlled trial. Obstetrics and Gynecology 2007;109:20‐7. - PubMed
References to ongoing studies
Additional references
Broder 2000
-
- Broder MS, Kanouse DE, Mittman BS, Bernstein SJ. The appropriateness of recommendations for hysterectomy in Southern California. Obstetrics and Gynaecology 2000;95(2):199‐205. - PubMed
Cardozo 2012
Coleman 2004
-
- Coleman P. Review body for interventional procedures, Sheffield: Commissioned by the National Institute for Clinical Excellence. National Institute for Clinical Excellence 2004.
Garry 2004
Gehlbach 1993
-
- Gehlbach DL, Sousa RC, Carpenter SE, Rock JA. Abdominal myomectomy in the treatment of infertility. International Journal of Gynaecology and Obstetrics 1993;40(1):45‐50. - PubMed
Goodwin 1997
-
- Goodwin S, Vendantham S, McLucas B, Forno A, Perella R. Preliminary experience with uterine fibroid embolization for uterine fibroids. Journal of Vascular and Interventional Radiology 1997;8:517‐26. - PubMed
Greenwood 1987
-
- Greenwood C, Glickman M, Schwartz P, Morse SS, Denny DF. Obstetric and non malignant gynecologic bleeding: Treatment with angiographic embolization radiology. Radiology 1987;164(1):155‐9. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
HOPEFUL 2007
-
- Dutton S, Hirst A, McPherson K, Nicholson T, Maresh M. A UK multicentre retrospective cohort study comparing hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids (HOPEFUL study): main results on medium‐term safety and efficacy. British Journal of Obstetrics and Gynaecology 2007;114:1340‐51. - PubMed
Khaund 2008
-
- Khaund A, Lumsden MA. Impact of fibroids on reproductive function. Best Practice & Research Clinical Obstetrics and Gynaecology 2008;22(4):749‐56. - PubMed
Lepine 1997
-
- Lepine LA, Hillis SD, Marchbanks PA, Koonin LM, Morrow B, Kicke BA, et al. Hysterectomy surveillance. United States 1980‐1983. Morbidity and Mortality Weekly Reports 1997;46 (SS‐4):1‐16. - PubMed
NCHS 1998
-
- National Centre for Health Statistics. Ambulatory and Inpatient Procedures in the United States, 1996. Hyattsville, Maryland: Public Health Service 1998; DHSS Publication No (PHS) 99‐1710.
NICE 2007
-
- National Institute for Health and Care Excellence. Heavy menstrual bleeding. http://www.nice.org.uk/guidance/cg44 (accessed 22 December 2014).
Okolo 2008
-
- Okolo S. Incidence, aetiology and epidemiology of uterine fibroids. Best Practice & Research Clinical Obstetrics and Gynaecology 2008;22(4):571–88. - PubMed
PEARL I
-
- Donnez J, Tatarchuk TF, Bouchard P, et al. Ulipristal acetate versus placebo for fibroid treatment before surgery. New England Journal of Medicine 2012;366(5):409‐20. - PubMed
PEARL II
-
- Donnez J, Tomaszewski J, Vázquez F. Ulipristal acetate versus leuprolide acetate for uterine fibroids. New England Journal of Medicine 2012;366(5):421‐32. - PubMed
Rahn 2011
Ravina 1997
-
- Ravina JH, Bouret JM, Ciraru‐Vigneron N, Repiqurt D, Herbreteau D, Aymard A, et al. Recourse to particular arterial embolization in the treatment of some uterine leiomyoma. Bulletin de Academie Nationale de Medecine 1997;181(2):233‐43. - PubMed
Spies 1999
-
- Spies JB, Warren EH, Mathias SD, Walsh SM, Roth AR, Pentecost MJ. Uterine fibroid embolization: measurement of health‐related quality of life before and after therapy. Journal of Vascular and Interventional Radiology 1999;10(10):1293‐303. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous