

Higher achieved mean arterial pressure during therapeutic hypothermia is not associated with neurologically intact survival following cardiac arrest
- PMID: 25541429
- PMCID: PMC4330116
- DOI: 10.1016/j.resuscitation.2014.12.008
Higher achieved mean arterial pressure during therapeutic hypothermia is not associated with neurologically intact survival following cardiac arrest
Abstract
Introduction: To determine if higher achieved mean arterial blood pressure (MAP) during treatment with therapeutic hypothermia (TH) is associated with neurologically intact survival following cardiac arrest.
Methods: Retrospective analysis of a prospectively collected cohort of 188 consecutive patients treated with TH in the cardiovascular intensive care unit of an academic tertiary care hospital.
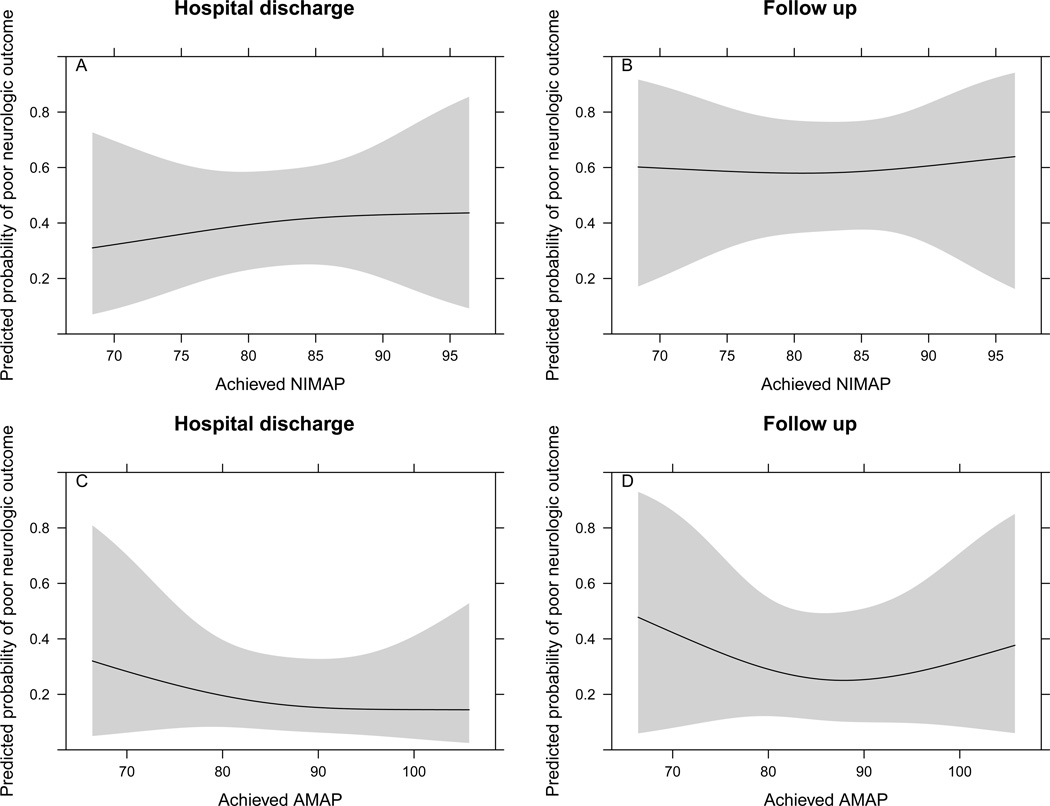
Results: Neurologically intact survival was observed in 73/188 (38.8%) patients at hospital discharge and in 48/162 (29.6%) patients at a median follow up interval of 3 months. Patients in shock at the time of admission had lower baseline MAP at the initiation of TH (81 versus 87mmHg; p=0.002), but had similar achieved MAP during TH (80.3 versus 83.7mmHg; p=0.11). Shock on admission was associated with poor survival (18% versus 52%; p<0.001). Vasopressor use among all patients was common (84.6%) and was not associated with increased mortality. A multivariable analysis including age, initial rhythm, time to return of spontaneous circulation, baseline MAP and achieved MAP did not demonstrate a relationship between MAP achieved during TH and poor neurological outcome at hospital discharge (OR 1.28, 95% CI 0.40-4.06; p=0.87) or at outpatient follow up (OR 1.09, 95% CI 0.32-3.75; p=0.976).
Conclusion: We did not observe a relationship between higher achieved MAP during TH and neurologically intact survival. However, shock at the time of admission was clearly associated with poor outcomes in our study population. These data do not support the use of vasopressors to artificially increase MAP in the absence of shock. There is a need for prospective, randomized trials to further define the optimum blood pressure target during treatment with TH.
Keywords: Cardiac arrest; Cerebral performance category; Mean arterial pressure; Shock; Therapeutic hypothermia.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics-2012 update: a report from the American Heart Association. Circulation. 2012;125(1):188–197. - PubMed
-
- Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, Gabrielli A, Silvers SM, Zaritsky AL, Merchant R, Vanden Hoek Kronick SL. Part 9: Post-Cardiac Arrest Care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18_suppl_3):S768–S786. - PubMed
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557–563. - PubMed
-
- Kern KB. Optimal Treatment of Patients Surviving Out-of-Hospital Cardiac Arrest. JACC Cardiovasc Interv. 2012;5(6):597–605. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
