

Four dimensional digital tomosynthesis using on-board imager for the verification of respiratory motion
- PMID: 25541710
- PMCID: PMC4277366
- DOI: 10.1371/journal.pone.0115795
Four dimensional digital tomosynthesis using on-board imager for the verification of respiratory motion
Abstract
Purpose: To evaluate respiratory motion of a patient by generating four-dimensional digital tomosynthesis (4D DTS), extracting respiratory signal from patients' on-board projection data, and ensuring the feasibility of 4D DTS as a localization tool for the targets which have respiratory movement.
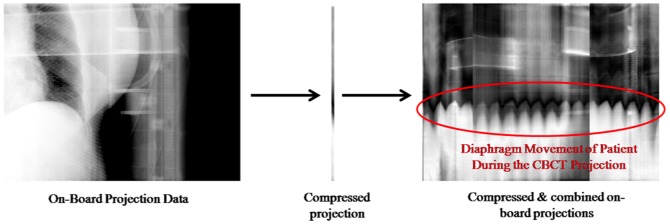
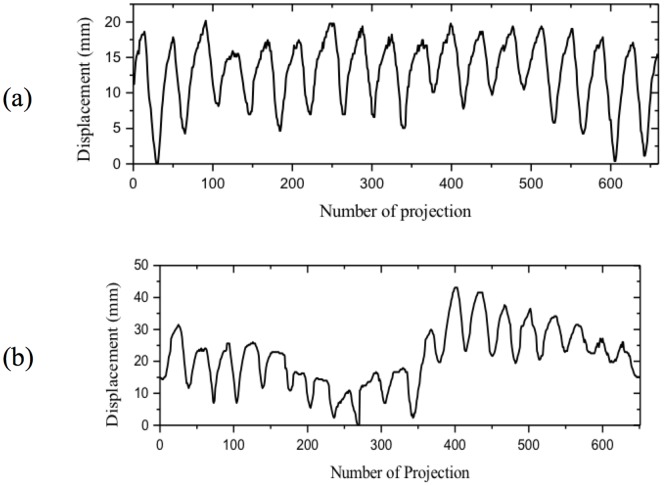
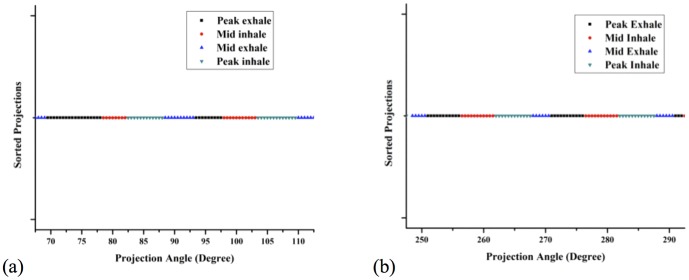
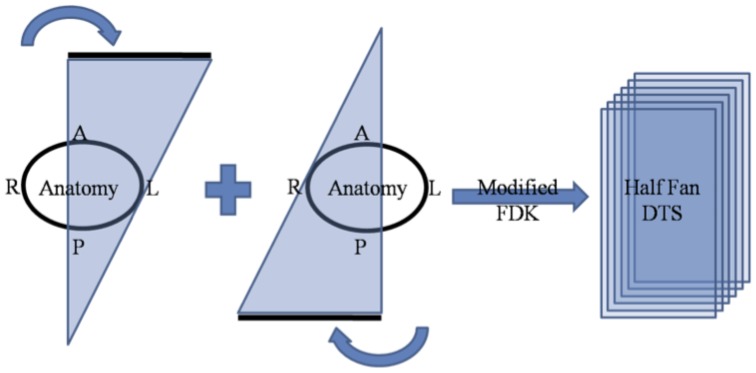
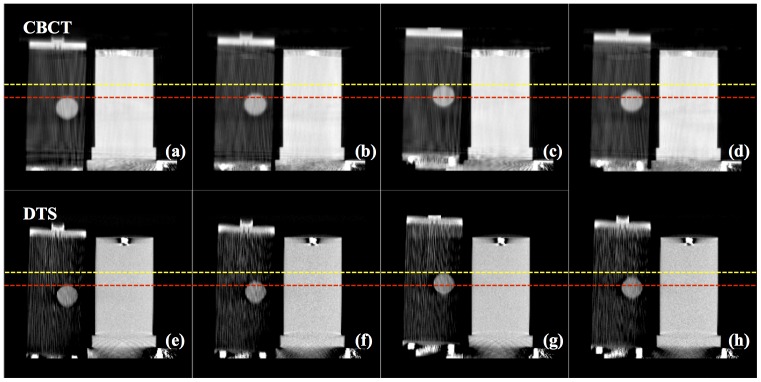
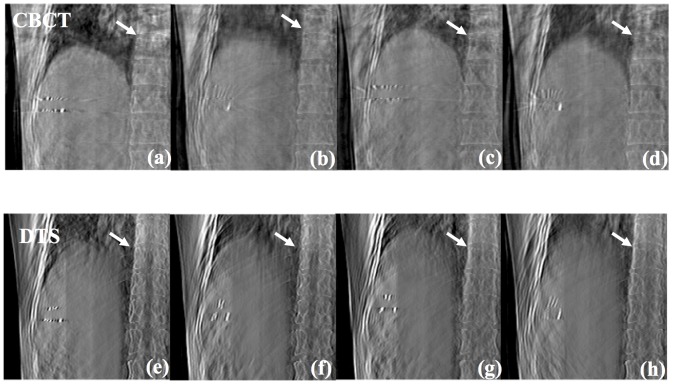
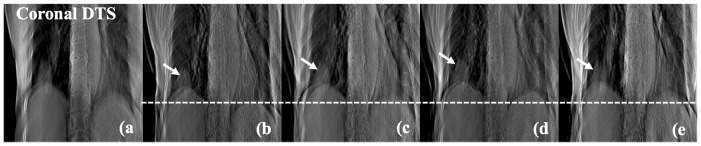
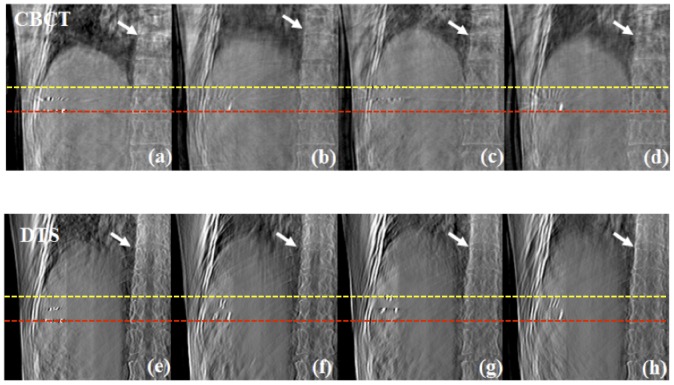
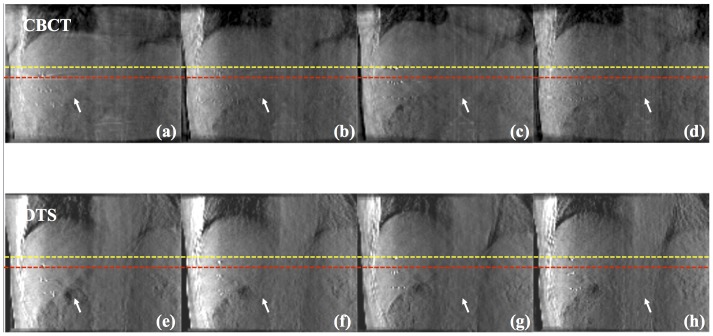
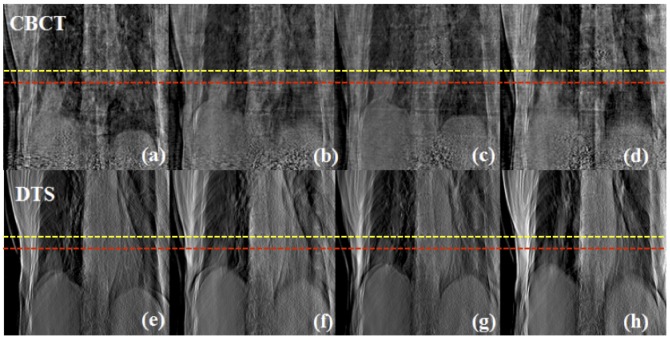
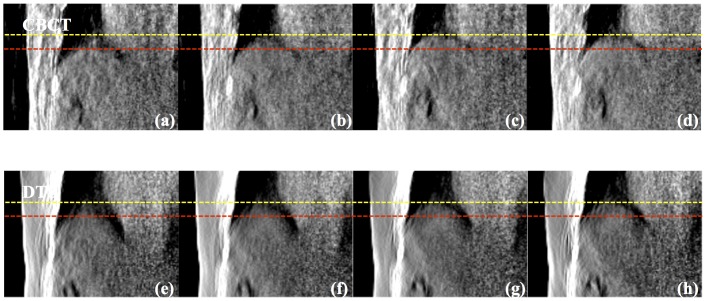
Methods and materials: Four patients with lung and liver cancer were included to verify the feasibility of 4D-DTS with an on-board imager. CBCT acquisition (650-670 projections) was used to reconstruct 4D DTS images and the breath signal of the patients was generated by extracting the motion of diaphragm during data acquisition. Based on the extracted signal, the projection data was divided into four phases: peak-exhale phase, mid-inhale phase, peak-inhale phase, and mid-exhale phase. The binned projection data was then used to generate 4D DTS, where the total scan angle was assigned as ±22.5° from rotation center, centered on 0° and 180° for coronal "half-fan" 4D DTS, and 90° and 270° for sagittal "half-fan" 4D DTS. The result was then compared with 4D CBCT which we have also generated with the same phase distribution.
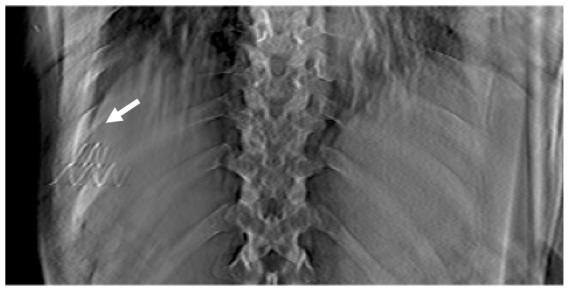
Results: The motion of the diaphragm was evident from the 4D DTS results for peak-exhale, mid-inhale, peak-inhale and mid-exhale phase assignment which was absent in 3D DTS. Compared to the result of 4D CBCT, the view aliasing effect due to arbitrary angle reconstruction was less severe. In addition, the severity of metal artifacts, the image distortion due to presence of metal, was less than that of the 4D CBCT results.
Conclusion: We have implemented on-board 4D DTS on patients data to visualize the movement of anatomy due to respiratory motion. The results indicate that 4D-DTS could be a promising alternative to 4D CBCT for acquiring the respiratory motion of internal organs just prior to radiotherapy treatment.
Conflict of interest statement
Figures
Similar articles
-
Slow gantry rotation acquisition technique for on-board four-dimensional digital tomosynthesis.Med Phys. 2010 Feb;37(2):921-33. doi: 10.1118/1.3285291. Med Phys. 2010. PMID: 20229901
-
On-board four-dimensional digital tomosynthesis: first experimental results.Med Phys. 2008 Aug;35(8):3574-83. doi: 10.1118/1.2953561. Med Phys. 2008. PMID: 18777918
-
Four-dimensional cone-beam computed tomography and digital tomosynthesis reconstructions using respiratory signals extracted from transcutaneously inserted metal markers for liver SBRT.Med Phys. 2011 Feb;38(2):1028-36. doi: 10.1118/1.3544369. Med Phys. 2011. PMID: 21452740
-
A technique for estimating 4D-CBCT using prior knowledge and limited-angle projections.Med Phys. 2013 Dec;40(12):121701. doi: 10.1118/1.4825097. Med Phys. 2013. PMID: 24320487
-
Simultaneous motion estimation and image reconstruction (SMEIR) for 4D cone-beam CT.Med Phys. 2013 Oct;40(10):101912. doi: 10.1118/1.4821099. Med Phys. 2013. PMID: 24089914
Cited by
-
Robust breathing signal extraction from cone beam CT projections based on adaptive and global optimization techniques.Phys Med Biol. 2016 Apr 21;61(8):3109-26. doi: 10.1088/0031-9155/61/8/3109. Epub 2016 Mar 23. Phys Med Biol. 2016. PMID: 27008349 Free PMC article.
-
Segmental analysis of respiratory liver motion in patients with and without a history of abdominal surgery.Jpn J Radiol. 2018 Aug;36(8):511-518. doi: 10.1007/s11604-018-0750-3. Epub 2018 Jun 20. Jpn J Radiol. 2018. PMID: 29922899
-
Optimising 4D imaging of fast-oscillating structures using X-ray microtomography with retrospective gating.Sci Rep. 2024 Sep 3;14(1):20499. doi: 10.1038/s41598-024-68684-1. Sci Rep. 2024. PMID: 39227377 Free PMC article.
-
A software tool of digital tomosynthesis application for patient positioning in radiotherapy.J Appl Clin Med Phys. 2016 Mar 8;17(2):174-193. doi: 10.1120/jacmp.v17i2.5999. J Appl Clin Med Phys. 2016. PMID: 27074482 Free PMC article.
-
Clinical Study of Orthogonal-View Phase-Matched Digital Tomosynthesis for Lung Tumor Localization.Technol Cancer Res Treat. 2017 Dec;16(6):866-878. doi: 10.1177/1533034617705716. Epub 2017 Apr 28. Technol Cancer Res Treat. 2017. PMID: 28449625 Free PMC article.
References
-
- Herman MG (2005) Clinical use of electronic portal imaging. Semin. Radiat. Oncol. 15:157–167. - PubMed
-
- Byrne TE (2005) A review of prostate motion with considerations for the treatment of prostate cancer. Med. Dosim. 30:155–161. - PubMed
-
- Kupelian PA, Lee C, Langen KM, Zeidan OA, Mawn RR, et al. (2008) Evaluation of image-guidance strategies in the treatment of localized prostate cancer. Int. J. Radiat. Oncol., Biol., Phys. 70:1151–1157. - PubMed
-
- Morin O, Gillis A, Chen J, Aubin M, Bucci MK, et al. (2006) Megavoltage cone-beam CT: System description and clinical applications. Med. Dosim. 31:51–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
