

Identification and predicting short-term prognosis of early cardiorenal syndrome type 1: KDIGO is superior to RIFLE or AKIN
- PMID: 25542014
- PMCID: PMC4277271
- DOI: 10.1371/journal.pone.0114369
Identification and predicting short-term prognosis of early cardiorenal syndrome type 1: KDIGO is superior to RIFLE or AKIN
Abstract
Objective: Acute kidney injury (AKI) in patients hospitalized for acute heart failure (AHF) is usually type 1 of the cardiorenal syndrome (CRS) and has been associated with increased morbidity and mortality. Early recognition of AKI is critical. This study was to determine if the new KDIGO criteria (Kidney Disease: Improving Global Outcomes) for identification and short-term prognosis of early CRS type 1 was superior to the previous RIFLE and AKIN criteria.
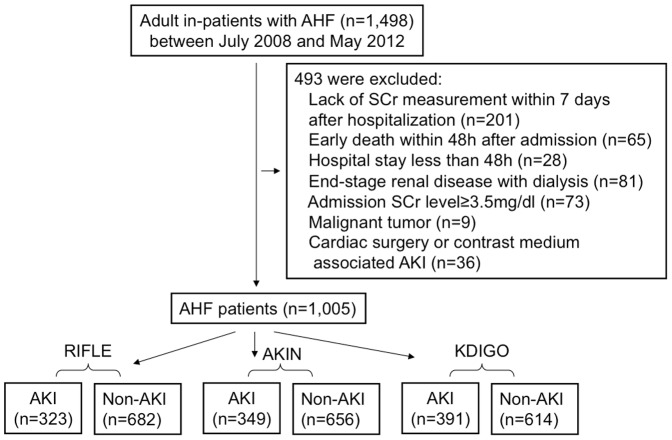
Methods: The association between AKI diagnosed by KDIGO but not by RIFLE or AKIN and in-hospital mortality was retrospectively evaluated in 1005 Chinese adult patients with AHF between July 2008 and May 2012. AKI was defined as RIFLE, AKIN and KDIGO criteria, respectively. Cox regression was used for multivariate analysis of in-hospital mortality.
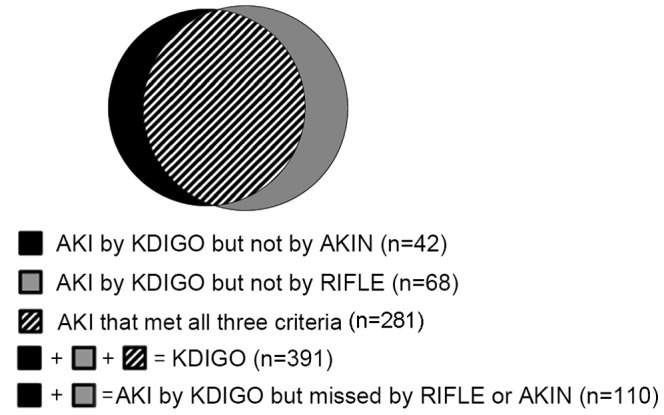
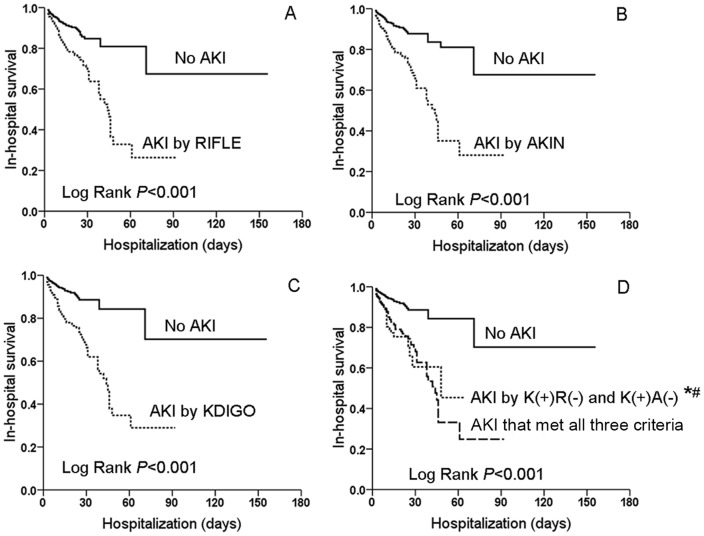
Results: Within 7 days on admission, the incidence of CRS type 1 was 38.9% by KDIGO criteria, 34.7% by AKIN, and 32.1% by RIFLE. A total of 110 (10.9%) cases were additional diagnosed by KDIGO criteria but not by RIFLE or AKIN. 89.1% of them were in Stage 1 (AKIN) or Stage Risk (RIFLE). They accounted for 18.4% (25 cases) of the overall death. After adjustment, this proportion remained an independent risk factor for in-hospital mortality [odds ratios (OR)3.24, 95% confidence interval(95%CI) 1.97-5.35]. Kaplan-Meier curve showed AKI patients by RIFLE, AKIN, KDIGO and [K(+)R(-)+K(+)A(-)] had lower hospital survival than non-AKI patients (Log Rank P<0.001).
Conclusion: KDIGO criteria identified significantly more CRS type 1 episodes than RIFLE or AKIN. AKI missed diagnosed by RIFLE or AKIN criteria was an independent risk factor for in-hospital mortality, indicating the new KDIGO criteria was superior to RIFLE and AKIN in predicting short-term outcomes in early CRS type 1.
Conflict of interest statement
Figures
Similar articles
-
A comparison of different diagnostic criteria of acute kidney injury in critically ill patients.Crit Care. 2014 Jul 8;18(4):R144. doi: 10.1186/cc13977. Crit Care. 2014. PMID: 25005361 Free PMC article.
-
Evaluation of acute kidney injury (AKI) with RIFLE, AKIN, CK, and KDIGO in critically ill trauma patients.Eur J Trauma Emerg Surg. 2018 Aug;44(4):597-605. doi: 10.1007/s00068-017-0820-8. Epub 2017 Jul 17. Eur J Trauma Emerg Surg. 2018. PMID: 28717983
-
Comparison of RIFLE, AKIN, and KDIGO classifications for assessing prognosis of patients on extracorporeal membrane oxygenation.J Formos Med Assoc. 2017 Nov;116(11):844-851. doi: 10.1016/j.jfma.2017.08.004. Epub 2017 Sep 2. J Formos Med Assoc. 2017. PMID: 28874330
-
Relationship between acute kidney injury and mortality in poisoning - a systematic review and metanalysis.Clin Toxicol (Phila). 2021 Sep;59(9):771-779. doi: 10.1080/15563650.2021.1928161. Epub 2021 Jun 3. Clin Toxicol (Phila). 2021. PMID: 34080503
-
Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria.BMC Nephrol. 2017 Feb 20;18(1):70. doi: 10.1186/s12882-017-0487-8. BMC Nephrol. 2017. PMID: 28219327 Free PMC article. Review.
Cited by
-
Pre-, Intra-, and Post-Operative Factors for Kidney Injury of Patients Underwent Cardiac Surgery: A Retrospective Cohort Study.Med Sci Monit. 2019 Aug 6;25:5841-5849. doi: 10.12659/MSM.915996. Med Sci Monit. 2019. PMID: 31383840 Free PMC article.
-
Decompensated Heart Failure and Renal Failure: What Is the Current Evidence?Curr Heart Fail Rep. 2018 Aug;15(4):224-238. doi: 10.1007/s11897-018-0397-5. Curr Heart Fail Rep. 2018. PMID: 29987499 Review.
-
A comprehensive review of acute cardio-renal syndrome: need for novel biomarkers.Front Pharmacol. 2023 May 23;14:1152055. doi: 10.3389/fphar.2023.1152055. eCollection 2023. Front Pharmacol. 2023. PMID: 37288107 Free PMC article. Review.
-
A new scoring model for the prediction of mortality in patients with acute kidney injury.Sci Rep. 2017 Aug 11;7(1):7862. doi: 10.1038/s41598-017-08440-w. Sci Rep. 2017. PMID: 28801674 Free PMC article.
-
Importance of sodium-glucose cotransporter 2 inhibitor use in diabetic patients with acute heart failure.Ther Adv Cardiovasc Dis. 2019 Jan-Dec;13:1753944719894509. doi: 10.1177/1753944719894509. Ther Adv Cardiovasc Dis. 2019. PMID: 31854243 Free PMC article.
References
-
- McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW (2004) Renal insufficiency and heart failure: prognostic and therapeutic implications from a prospective cohort study. Circulation. 109:1004–1009. - PubMed
-
- Cowie MR, Komajda M, Murray-Thomas T, Underwood J, Ticho B, et al. (2006) Prevalence and impact of worsening renal function in patients hospitalized with decompensated heart failure: results of the prospective outcomes study in heart failure (POSH). Eur Heart J. 27:1216–1222. - PubMed
-
- Shirakabe A, Hata N, Kobayashi N, Shinada T, Tomita K, et al. (2012) Long-term prognostic impact after acute kidney injury in patients with acute heart failure. Int Heart J. 53:313–319. - PubMed
-
- Ronco C, Cicoira M, McCullough PA (2012) Cardiorenal syndrome type 1: pathophysiological crosstalk leading to combined heart and kidney dysfunction in the setting of acutely decompensated heart failure. J Am Coll Cardiol. 60:1031–1042. - PubMed
-
- Haase M, Müller C, Damman K, Murray PT, Kellum JA, et al. (2013) Pathogenesis of cardiorenal syndrome type 1 in acute decompensated heart failure: workgroup statements from the eleventh consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol. 182:99–116. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
