

Maternal obesity and occurrence of fetal macrosomia: a systematic review and meta-analysis
- PMID: 25544943
- PMCID: PMC4273542
- DOI: 10.1155/2014/640291
Maternal obesity and occurrence of fetal macrosomia: a systematic review and meta-analysis
Abstract
Objective: To determine a precise estimate for the contribution of maternal obesity to macrosomia.
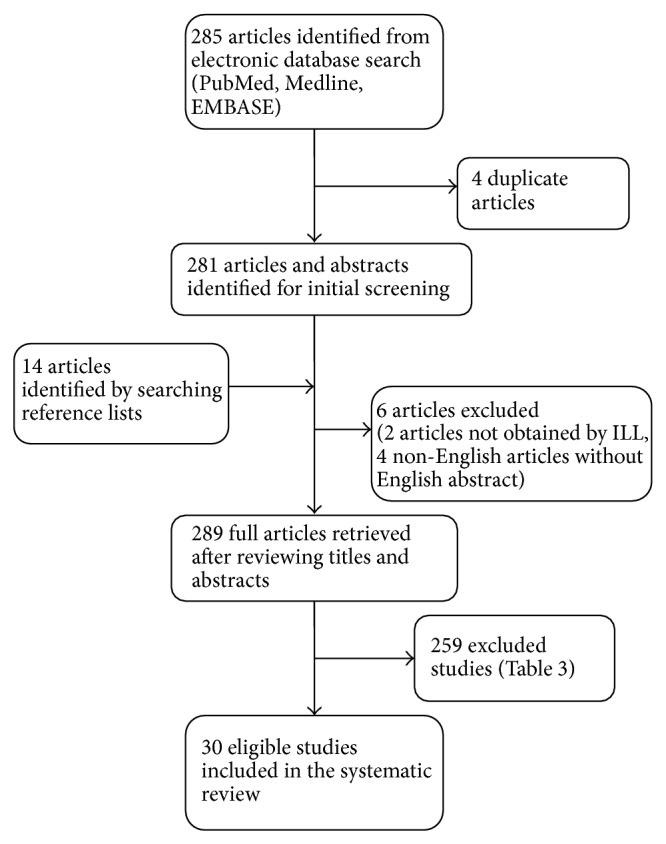
Data sources: The search strategy included database searches in 2011 of PubMed, Medline (In-Process & Other Non-Indexed Citations and Ovid Medline, 1950-2011), and EMBASE Classic + EMBASE. Appropriate search terms were used for each database. Reference lists of retrieved articles and review articles were cross-referenced.
Methods of study selection: All studies that examined the relationship between maternal obesity (BMI ≥30 kg/m(2)) (pregravid or at 1st prenatal visit) and fetal macrosomia (birth weight ≥4000 g, ≥4500 g, or ≥90th percentile) were considered for inclusion.
Tabulation, integration, and results: Data regarding the outcomes of interest and study quality were independently extracted by two reviewers. Results from the meta-analysis showed that maternal obesity is associated with fetal overgrowth, defined as birth weight ≥ 4000 g (OR 2.17, 95% CI 1.92, 2.45), birth weight ≥4500 g (OR 2.77,95% CI 2.22, 3.45), and birth weight ≥90% ile for gestational age (OR 2.42, 95% CI 2.16, 2.72).
Conclusion: Maternal obesity appears to play a significant role in the development of fetal overgrowth. There is a critical need for effective personal and public health initiatives designed to decrease prepregnancy weight and optimize gestational weight gain.
Figures



References
-
- Bérard J., Dufour P., Vinatier D., Subtil D., Vanderstichèle S., Monnier J. C., Puech F. Fetal macrosomia: risk factors and outcome. A study of the outcome concerning 100 cases >4500 g. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1998;77(1):51–59. doi: 10.1016/S0301-2115(97)00242-X. - DOI - PubMed
-
- Surkan P. J., Hsieh C.-C., Johansson A. L. V., Dickman P. W., Cnattingius S. Reasons for increasing trends in large for gestational age births. Obstetrics and Gynecology. 2004;104(4):720–726. doi: 10.1097/01.AOG.0000141442.59573.cd. - DOI - PubMed
-
- Khashu M., Pelligra G., Bhargava S., Smyth J. A. Perinatal Morbidity in Macrosomic Infants. Pediatric Academy of Sciences; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
