

Material need insecurities, control of diabetes mellitus, and use of health care resources: results of the Measuring Economic Insecurity in Diabetes study
- PMID: 25545780
- PMCID: PMC4484589
- DOI: 10.1001/jamainternmed.2014.6888
Material need insecurities, control of diabetes mellitus, and use of health care resources: results of the Measuring Economic Insecurity in Diabetes study
Abstract
Importance: Increasing access to care may be insufficient to improve the health of patients with diabetes mellitus and unmet basic needs (hereinafter referred to as material need insecurities). How specific material need insecurities relate to clinical outcomes and the use of health care resources in a setting of near-universal access to health care is unclear.
Objective: To determine the association of food insecurity, cost-related medication underuse, housing instability, and energy insecurity with control of diabetes mellitus and the use of health care resources.
Design, setting, and participants: Cross-sectional data were collected from June 1, 2012, through October 31, 2013, at 1 academic primary care clinic, 2 community health centers, and 1 specialty center for the treatment of diabetes mellitus in Massachusetts. A random sample of 411 patients, stratified by clinic, consisted of adults (aged ≥21 years) with diabetes mellitus (response rate, 62.3%).
Main outcomes and measures: The prespecified primary outcome was a composite indicator of poor diabetes control (hemoglobin A1c level, >9.0%; low-density lipoprotein cholesterol level, >100 mg/dL; or blood pressure, >140/90 mm Hg). Prespecified secondary outcomes included outpatient visits and a composite of emergency department (ED) visits and acute care hospitalizations (ED/inpatient visits).
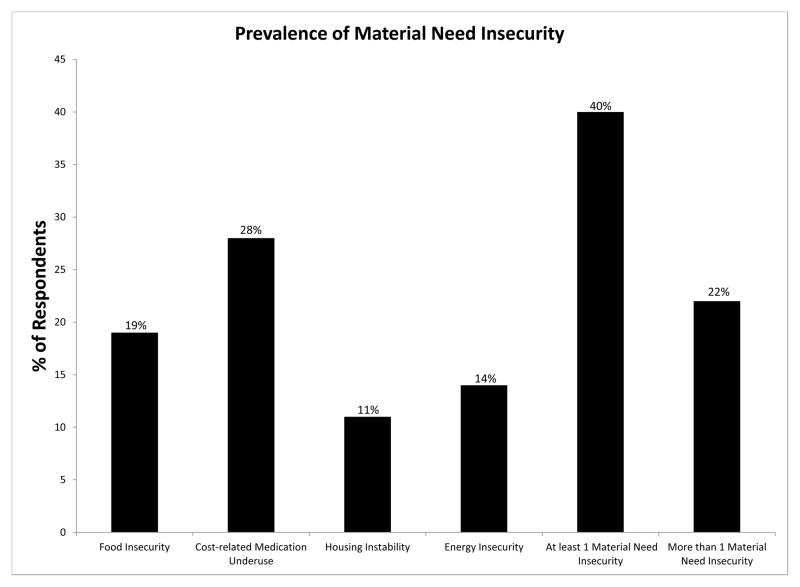
Results: Overall, 19.1% of respondents reported food insecurity; 27.6%, cost-related medication underuse; 10.7%, housing instability; 14.1%, energy insecurity; and 39.1%, at least 1 material need insecurity. Poor diabetes control was observed in 46.0% of respondents. In multivariable models, food insecurity was associated with a greater odds of poor diabetes control (adjusted odds ratio [OR], 1.97 [95% CI, 1.58-2.47]) and increased outpatient visits (adjusted incident rate ratio [IRR], 1.19 [95% CI, 1.05-1.36]) but not increased ED/inpatient visits (IRR, 1.00 [95% CI, 0.51-1.97]). Cost-related medication underuse was associated with poor diabetes control (OR, 1.91 [95% CI, 1.35-2.70]) and increased ED/inpatient visits (IRR, 1.68 [95% CI, 1.21-2.34]) but not outpatient visits (IRR, 1.07 [95% CI, 0.95-1.21]). Housing instability (IRR, 1.31 [95% CI, 1.14-1.51]) and energy insecurity (IRR, 1.12 [95% CI, 1.00-1.25]) were associated with increased outpatient visits but not with diabetes control (OR, 1.10 [95% CI, 0.60-2.02] and OR, 1.27 [95% CI, 0.96-1.69], respectively) or with ED/inpatient visits (IRR, 1.49 [95% CI, 0.81-2.73] and IRR, 1.31 [95% CI, 0.80-2.13], respectively). An increasing number of insecurities was associated with poor diabetes control (OR for each additional need, 1.39 [95% CI, 1.18-1.63]) and increased use of health care resources (IRR for outpatient visits, 1.09 [95% CI, 1.03-1.15]; IRR for ED/inpatient visits, 1.22 [95% CI, 0.99-1.51]).
Conclusions and relevance: Material need insecurities were common among patients with diabetes mellitus and had varying but generally adverse associations with diabetes control and the use of health care resources. Material need insecurities may be important targets for improving care of diabetes mellitus.
Conflict of interest statement
Conflict of Interest Disclosures: All authors declare they have no conflicts of interest to report.
Figures
References
-
- [Accessed 17 Mar 2014];The Patient Protection and Affordable Care Act, P.L. 111–148. 2010 Mar 23; http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf.
-
- Pincus T, Esther R, DeWalt DA, Callahan LF. Social conditions and self-management are more powerful determinants of health than access to care. Ann Intern Med. 1998 Sep 1;129(5):406–411. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
